

Trauma Embolic Scoring System in military trauma: a sensitive predictor of venous thromboembolism
- PMID: 31897437
- PMCID: PMC6924724
- DOI: 10.1136/tsaco-2019-000367
Trauma Embolic Scoring System in military trauma: a sensitive predictor of venous thromboembolism
Abstract
Introduction: Clinical decision support tools capable of predicting which patients are at highest risk for venous thromboembolism (VTE) can assist in guiding surveillance and prophylaxis decisions. The Trauma Embolic Scoring System (TESS) has been shown to model VTE risk in civilian trauma patients. No such support tools have yet been described in combat casualties, who have a high incidence of VTE. The purpose of this study was to evaluate the utility of TESS in predicting VTE in military trauma patients.
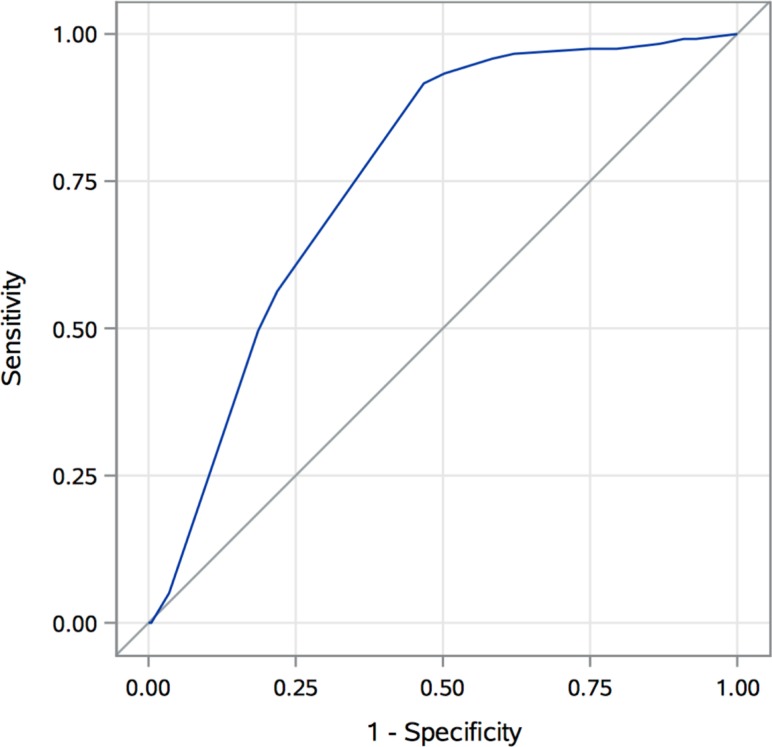
Methods: A retrospective cohort study of 549 combat casualties from October 2010 to November 2012 admitted to a military treatment facility in the USA was performed. TESS scores were calculated through data obtained from the Department of Defense Trauma Registry and chart reviews. Univariate analysis and multivariate logistic regression were performed to evaluate risk factors for VTE. Receiver operating characteristic (ROC) curve analysis of TESS in military trauma patients was also performed.
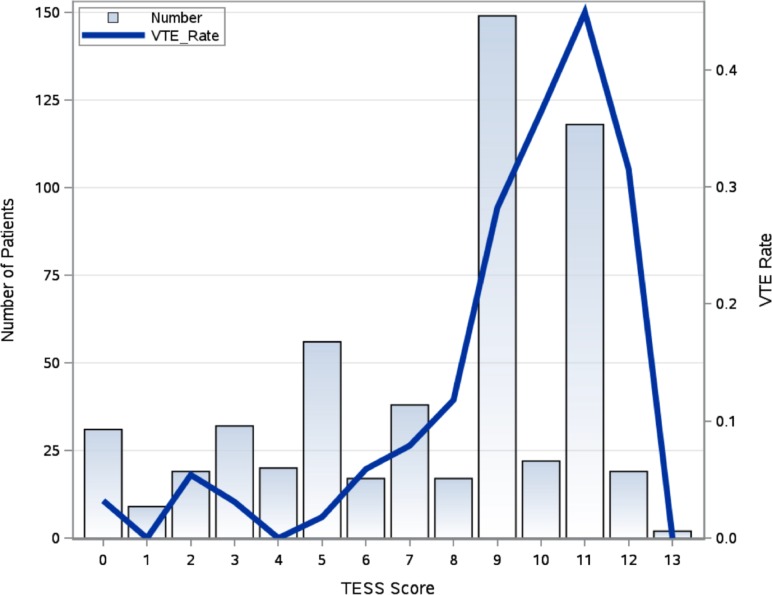
Results: The incidence of VTE was 21.7% (119/549). The median TESS for patients without VTE was 8 (IQR 4-9), and the median TESS for those with VTE was 10 (IQR 9-11). On multivariate analysis, Injury Severity Score (ISS) (OR 1.03, p=0.007), ventilator days (OR 1.05, p=0.02), and administration of tranexamic acid (TXA) (OR 1.89, p=0.03) were found to be independent risk factors for development of VTE. On ROC analysis, an optimal high-risk cut-off value for TESS was ≥7 with a sensitivity of 0.92 and a specificity of 0.53 (area under the curve 0.76, 95% CI 0.72 to 0.80, p<0.0001).
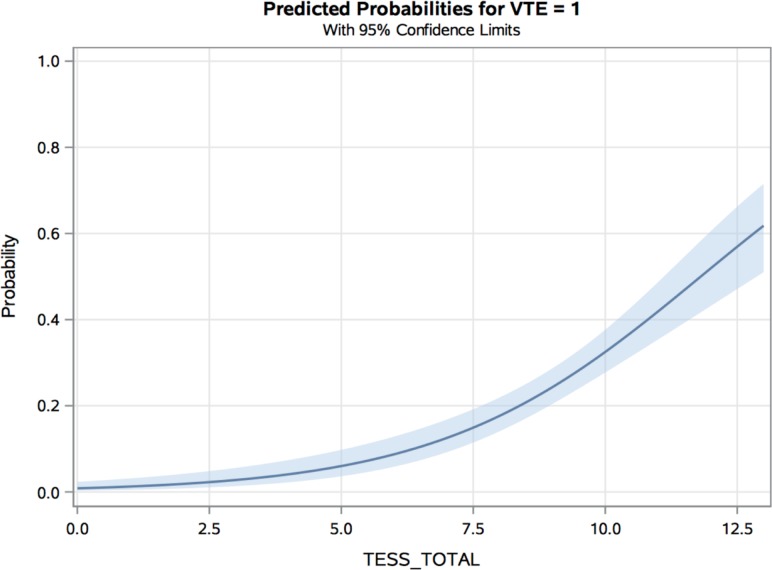
Conclusions: When used to predict VTE in military trauma, TESS shows moderate discrimination and is well calibrated. An optimal high-risk cut-off value of ≥7 demonstrates high sensitivity in predicting VTE. In addition to ISS and ventilator days, TXA administration is an independent risk factor for VTE development.
Level of evidence: Level III.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Knudson MM, Gomez D, Haas B, Cohen MJ, Nathens AB. Three thousand seven hundred thirty-eight posttraumatic pulmonary emboli: a new look at an old disease. Ann Surg 2011;254:632. - PubMed
-
- Fang R, Rodriguez CJ. Venous thromboembolism among military combat casualties. Curr Trauma Rep 2016;2:48–53. 10.1007/s40719-016-0037-z - DOI
LinkOut - more resources
Full Text Sources
Research Materials