

Use of FEF25-75% to Guide IgG Dosing to Protect Pulmonary Function in CVID
- PMID: 31897777
- PMCID: PMC8675332
- DOI: 10.1007/s10875-019-00730-4
Use of FEF25-75% to Guide IgG Dosing to Protect Pulmonary Function in CVID
Abstract
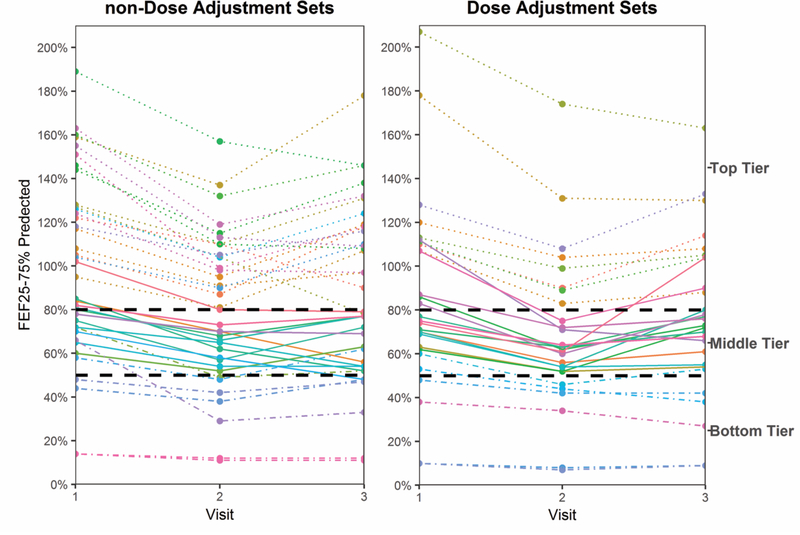
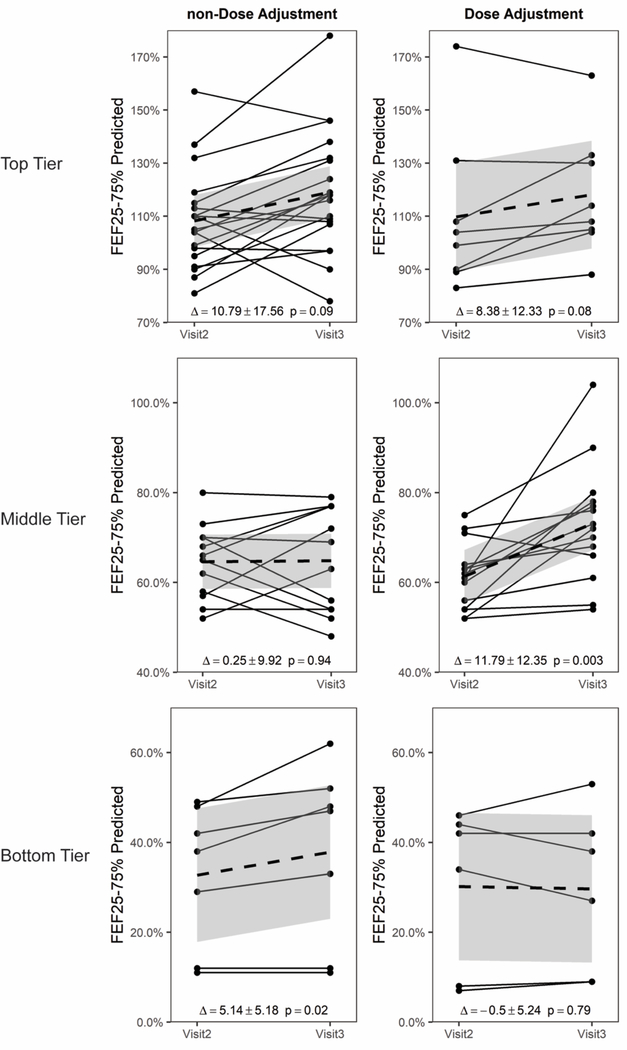
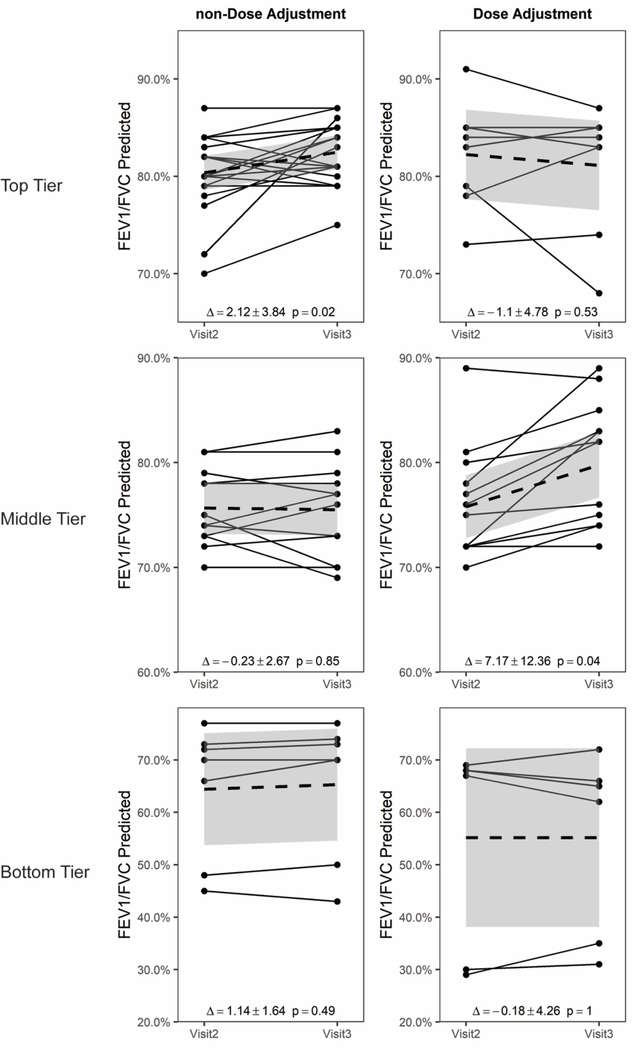
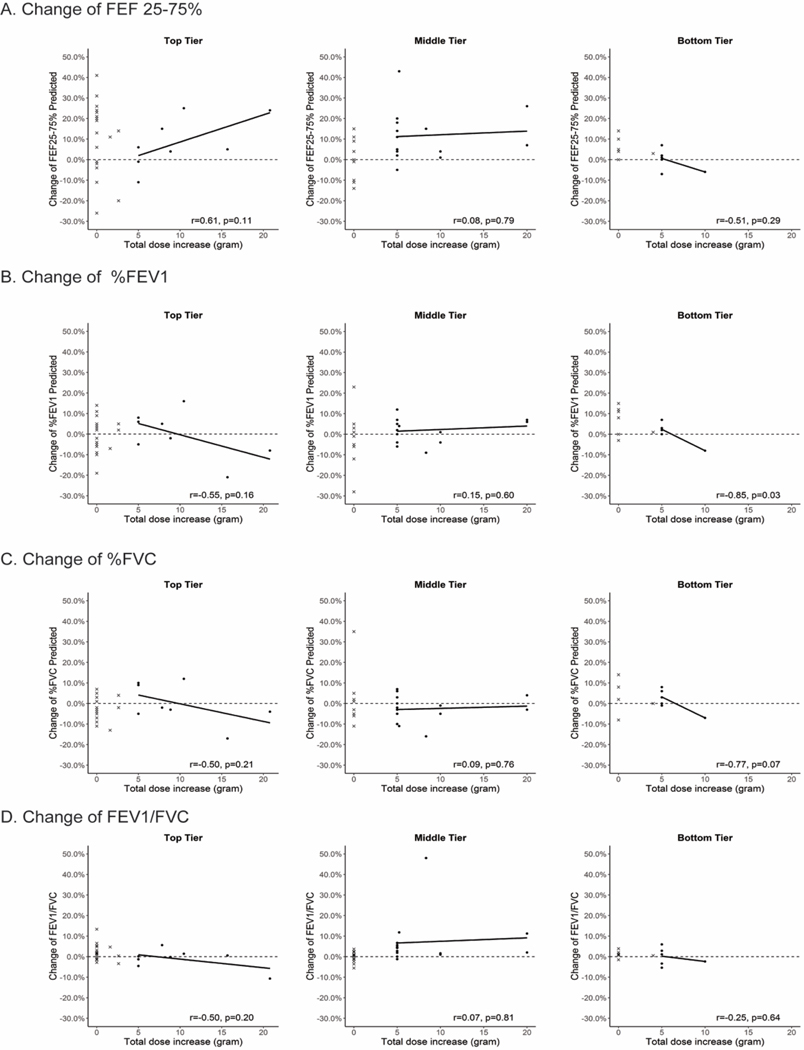
Immunoglobulin replacement therapy (IGRT) can protect against lung function decline in CVID. We tested whether increasing IgG dosage was beneficial in patients who exhibited a decline in forced expiratory flow at 25-75% (FEF25-75%) even though they were receiving IgG doses within the therapeutic range. Of 189 CVID patients seen over 12 years, 38 patients met inclusion criteria, were seen on ≥ 3 visits, and demonstrated a ≥ 10% decrease in FEF25-75% from visits 1 to 2. FEF25-75%, forced expiratory flow at 1 s (FEV1), and FEV1/FVC at visit 3 were compared among those with non-dose adjustment (non-DA) versus additional IgG dose adjustment (DA). Three FEF25-75% tiers were identified: top (> 80% predicted), middle (50-80%), and bottom (< 50%). DA and non-DA groups did not differ in clinical infections or bronchodilator use, although the non-DA group tended to use more antibiotics. In the top, normal tier, FEF25-75% increased in DA, but the change did not achieve statistical significance. In the middle moderate obstruction tier, visit 3 FEF25-75% increased among DA but not non-DA sets (11.8 ± 12.4%, p = 0.003 vs. 0.3 ± 9.9%, p = 0.94). Improvement in FEV1/FVC at visit 3 was also significant among DA vs. non-DA (7.2 ± 12.4%, p = 0.04 vs. - 0.2 ± 2.7%, p = 0.85). In the bottom, severe tier, FEF25-75% was unchanged in DA (- 0.5 ± 5.2%, p = 0.79), but increased in non-DA (5.1 ± 5.2%, p = 0.02). Among IGRT CVID patients with moderate but not severe obstruction as assessed by spirometry, increasing IgG dosage led to an increase in FEF25-75% and FEV1/FVC.
Keywords: Common variable immunodeficiency (CVID); FEF25–75%; IgG dose adjustment; Immunoglobulin replacement therapy; Prophylactic antibiotics; Spirometry.
Conflict of interest statement
Figures
References
-
- Schroeder HW Jr. , Schroeder HW, III, Sheikh SM. The complex genetics of common variable immunodeficiency. Journal of Investigative Medicine. 2004;52(2):90–103. - PubMed
-
- Cunningham-Rundles C, Siegal FP, Smithwick EM, Lion-Boule A, Cunningham-Rundles S, O’Malley J et al. Efficacy of intravenous immunoglobulin in primary humoral immunodeficiency disease. Annals of internal medicine. 1984;101(4):435–9. - PubMed
-
- Busse PJ, Razvi S, Cunningham-Rundles C. Efficacy of intravenous immunoglobulin in the prevention of pneumonia in patients with common variable immunodeficiency. J Allergy Clin Immunol. 2002;109(6):1001–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
