

Short-Term VA Health Care Expenditures Following a Health Risk Assessment and Coaching Trial
- PMID: 31898118
- PMCID: PMC7210324
- DOI: 10.1007/s11606-019-05455-z
Short-Term VA Health Care Expenditures Following a Health Risk Assessment and Coaching Trial
Abstract
Background: Short-term health care costs following completion of health risk assessments and coaching programs in the VA have not been assessed.
Objective: To compare VA health care expenditures among veterans who participated in a behavioral intervention trial that randomized patients to complete a HRA followed by health coaching (HRA + coaching) or to complete the HRA without coaching (HRA-alone).
Design: Four-hundred seventeen veterans at three Veterans Affairs (VA) Medical Centers or Clinics were randomized to HRA + coaching or HRA-alone. Veterans randomized to HRA-alone (n = 209) were encouraged to discuss HRA results with their primary care team, while veterans randomized to HRA + coaching (n = 208) received two brief telephone-delivered health coaching calls.
Participants: We included 411 veterans with available cost data.
Main measures: Total VA health expenditures 6 months following trial enrollment were estimated using a generalized linear model with a gamma distribution and log link function. In exploratory analysis, model-based recursive partitioning was used to determine whether the intervention effect on short-term costs differed among any patient subgroups.
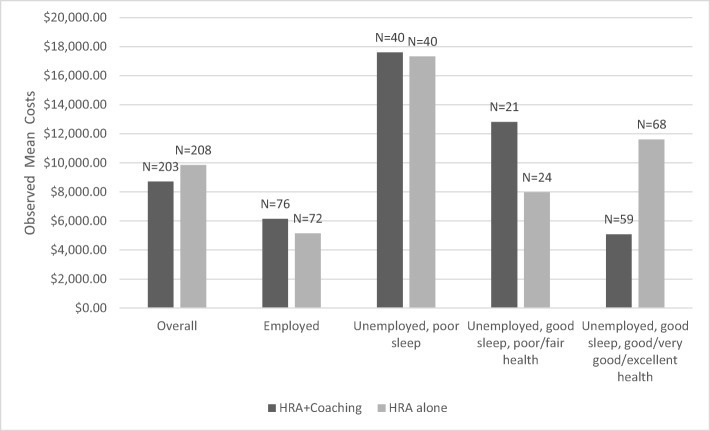
Key results: Most participants were male (85%); mean age was 56, and mean body mass index was 34. From the generalized linear model, 6-month estimated mean total VA expenditures were similar ($8665 for HRA + coaching vs $9900 for HRA-alone, p = 0.25). In exploratory subgroup analysis, among unemployed veterans with good sleep and fair or poor perceived health, mean observed expenditures in the HRA + coaching group were higher than in the HRA-alone group ($12,814 vs $7971). Among unemployed veterans with good sleep and good general health, mean observed expenditures in the HRA + coaching group were lower than in the HRA-alone group ($5082 vs $11,612).
Conclusions: Compared to completing and receiving HRA results, working with health coaches to set actionable health behavior change goals following HRA completion did not reduce short-term health expenditures.
Trial registration: Clinicaltrials.gov identifier: NCT01828567.
Keywords: behavioral; expenditures; health care costs; veterans.
Conflict of interest statement
Dr. Maciejewski owns Amgen stock due to his spouse's employment. All other authors have no conflicts.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
