

Determining Clinically Based Factors Associated With Reclassification in the Pre-MRI Era using a Large Prospective Active Surveillance Cohort
- PMID: 31899230
- PMCID: PMC7141963
- DOI: 10.1016/j.urology.2019.11.041
Determining Clinically Based Factors Associated With Reclassification in the Pre-MRI Era using a Large Prospective Active Surveillance Cohort
Abstract
Objective: To report biopsy-related and oncologic outcomes in a large prospective active surveillance cohort that was initiated in the premagnetic resonance imaging era and to additionally identify clinical factors associated with disease reclassification in order to inform future studies designed to improve enrollment and follow-up on active surveillance.
Methods: Patients were prospectively enrolled at a single institution from 2006 to 2014 and followed until 2016. Men with Gleason 6 or 7 disease were eligible, and those with >6 months follow-up were included in the analysis. Patients were risk stratified based on clinical/pathologic criteria, including based on a combination of baseline and confirmatory biopsy tumor characteristics. Reclassification-free survival, based on tumor volume increase or Gleason score increase, was analyzed using multivariable Cox proportional hazards models.
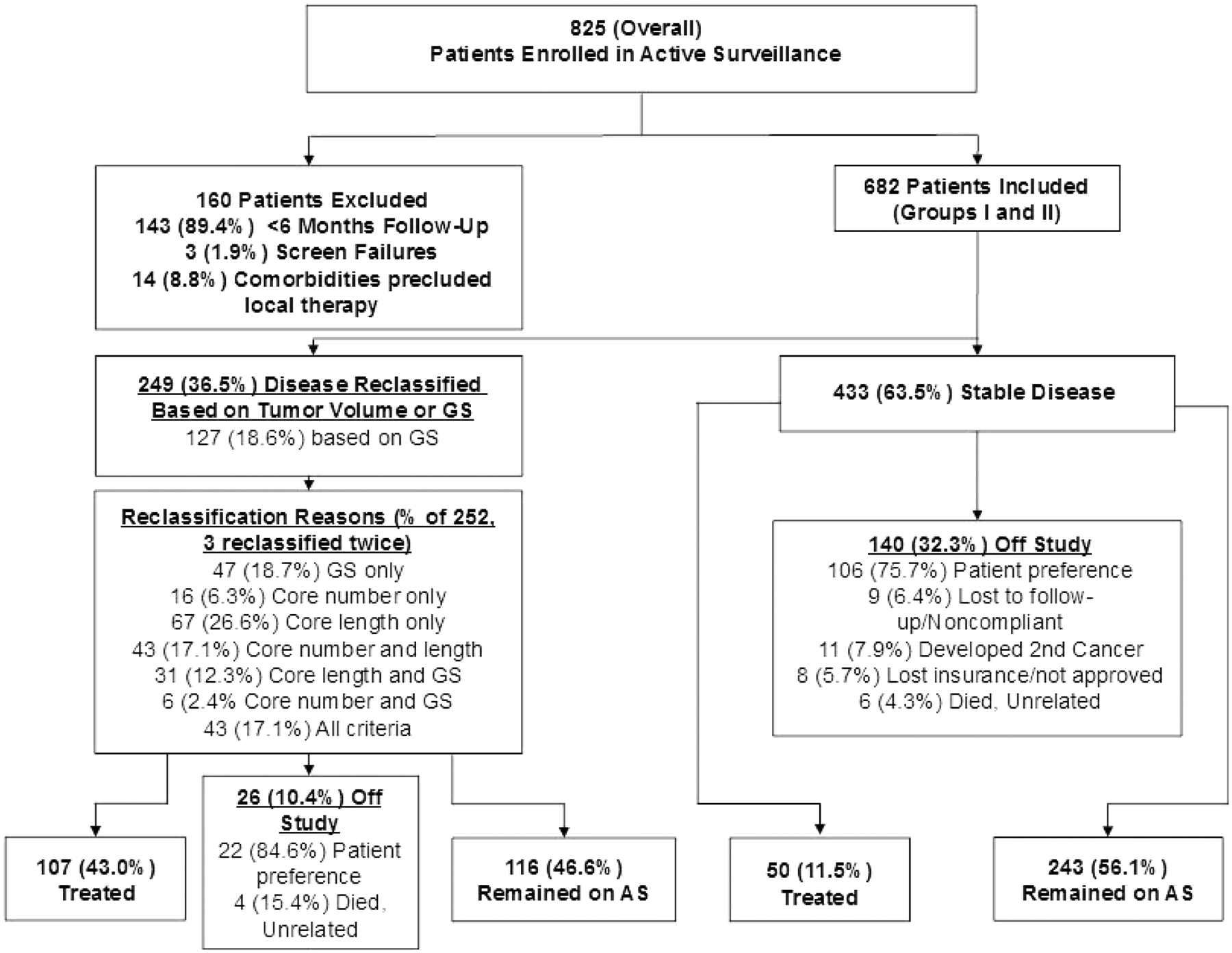
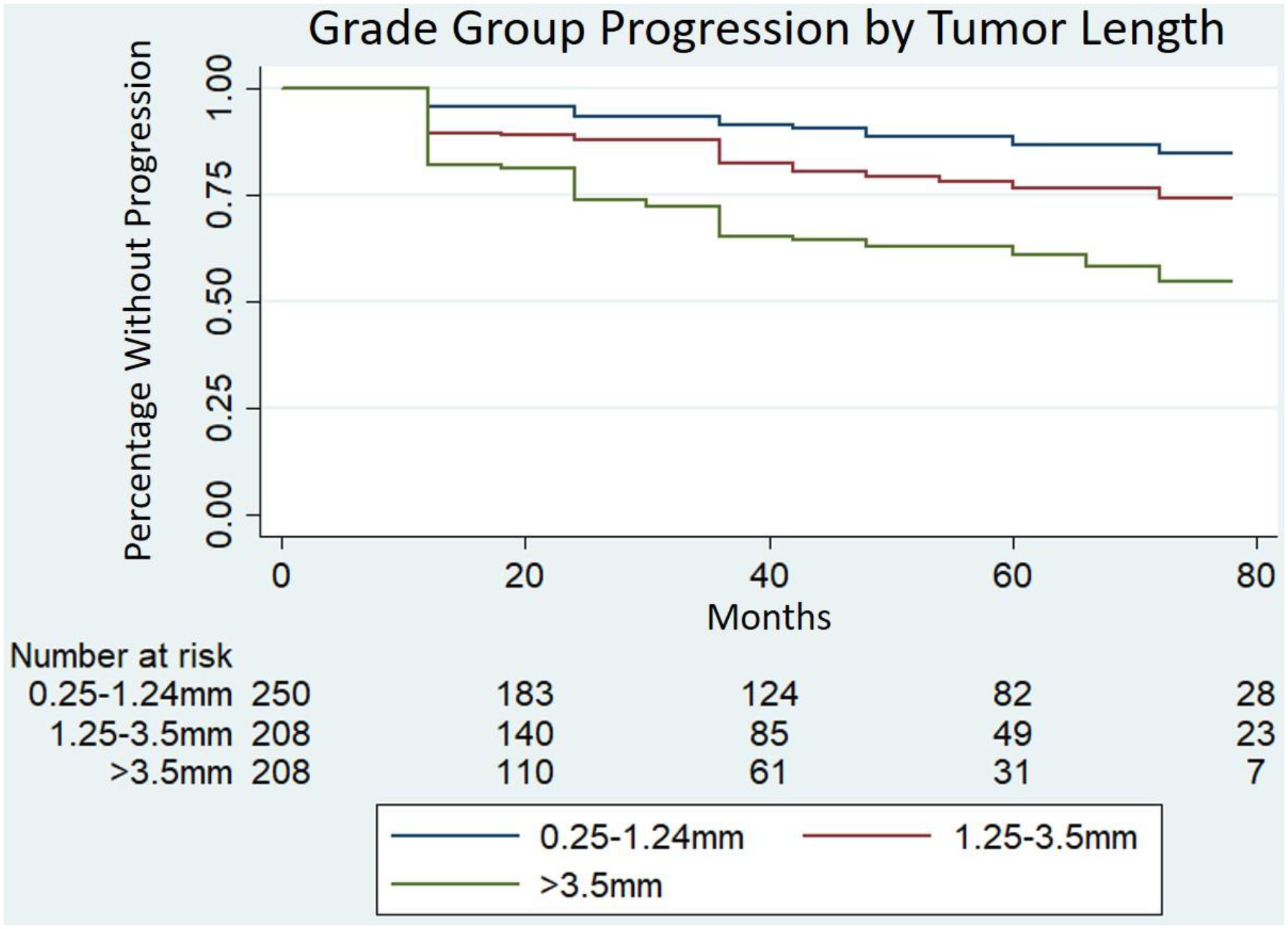
Results: Of 825 enrolled patients, 682 met inclusion criteria. Median follow-up was 40 months (range 6.6-126.8). Disease was reclassified in 249 (36.5%), and 157 (23.0%) underwent treatment. A single positive core with a negative confirmatory biopsy was significantly associated with time to reclassification (median not met vs 43 months, log rank test P <.001). Composite tumor length, defined as the combined tumor length between baseline and confirmatory biopsies, was associated with shorter Gleason upgrade-free survival (hazard ratio 1.24, 95% confidence interval 1.11-1.40, P <.001) in multivariable analysis.
Conclusion: Baseline stratification using clinical factors including tumor length may refine risk stratification and offer the foundation on which new systems that incorporate modalities such as magnetic resonance imaging may be based.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Comment in
-
EDITORIAL COMMENT.Urology. 2020 Apr;138:97. doi: 10.1016/j.urology.2019.11.057. Urology. 2020. PMID: 32252959 No abstract available.
References
-
- Barocas DA, Cowan JE, Smith JA, Carroll PR, CaPSURE Investigators. What percentage of patients with newly diagnosed carcinoma of the prostate are candidates for surveillance? An analysis of the CaPSURE database. J Urol. 2008;180(4):1330–1334; discussion 1334–1335. doi:10.1016/j.juro.2008.06.019 - DOI - PubMed
-
- Mohler JL, Armstrong AJ, Bahnson RR, et al. Prostate Cancer, Version 1.2016. J Natl Compr Cancer Netw JNCCN. 2016;14(1):19–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
