

Association between immunosuppressive cytokines and PSA progression in biochemically recurrent prostate cancer treated with intermittent hormonal therapy
- PMID: 31899823
- PMCID: PMC6980998
- DOI: 10.1002/pros.23948
Association between immunosuppressive cytokines and PSA progression in biochemically recurrent prostate cancer treated with intermittent hormonal therapy
Abstract
Background: Immunosuppressive cytokines have the potential to promote prostate cancer progression. Assessing their longitudinal changes may implicate mechanisms of progression, treatment resistance, and suggest new therapeutic targets.
Methods: Thirty-seven men with biochemically recurrent (BCR) prostate cancer who received 6 months of androgen deprivation therapy (ADT) and were monitored until the time to prostate-specific antigen progression (TTPP) were identified from a completed phase III trial (NCT00020085). Serum samples were archived at baseline, 3 months after ADT, and at TTPP. Cytokine concentrations were quantified using a 36-parameter electrochemiluminescence assay. The Wilcoxon signed-rank sum test was used to compare observations between time points. Kaplan-Meier analysis was used to calculate TTPP dichotomized by cytokine values above or below the median. Pearson's rank correlation coefficient was used to compare continuous variables.
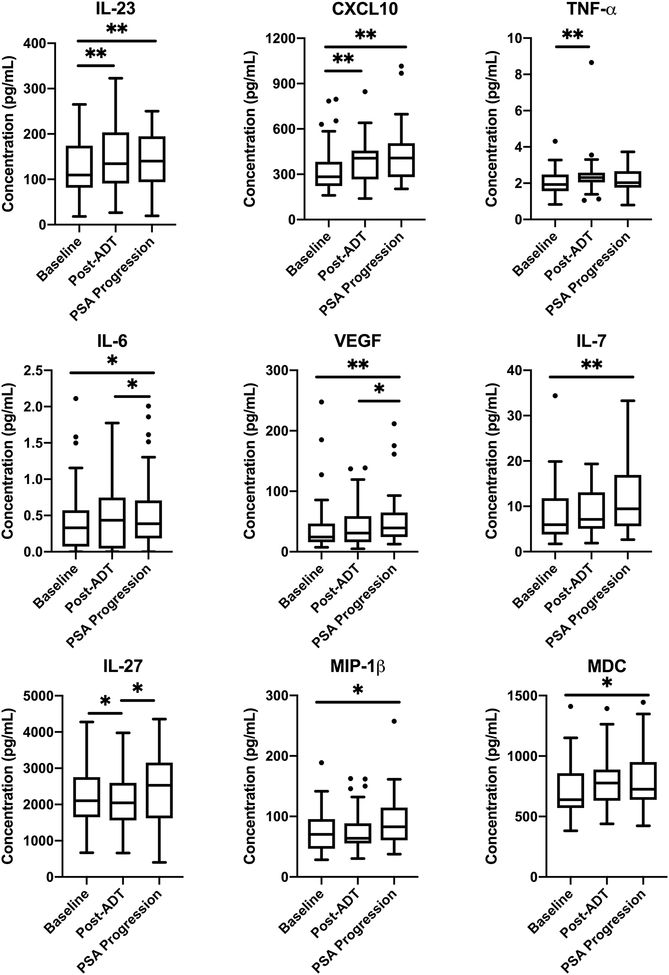
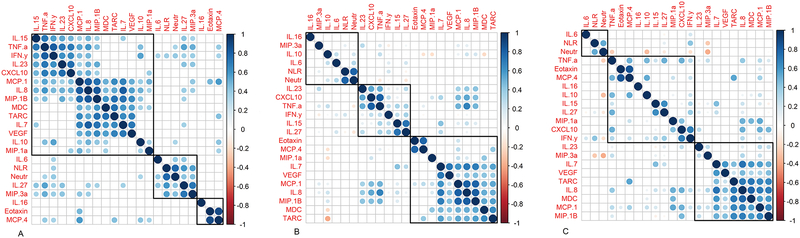
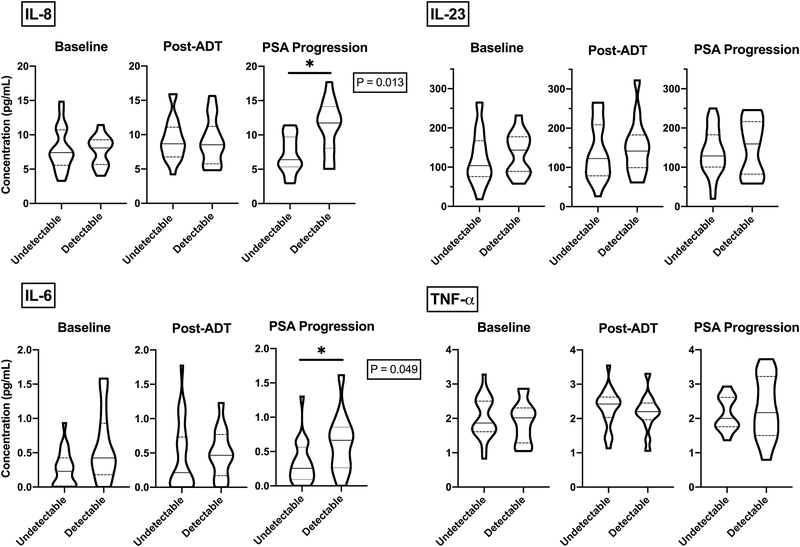
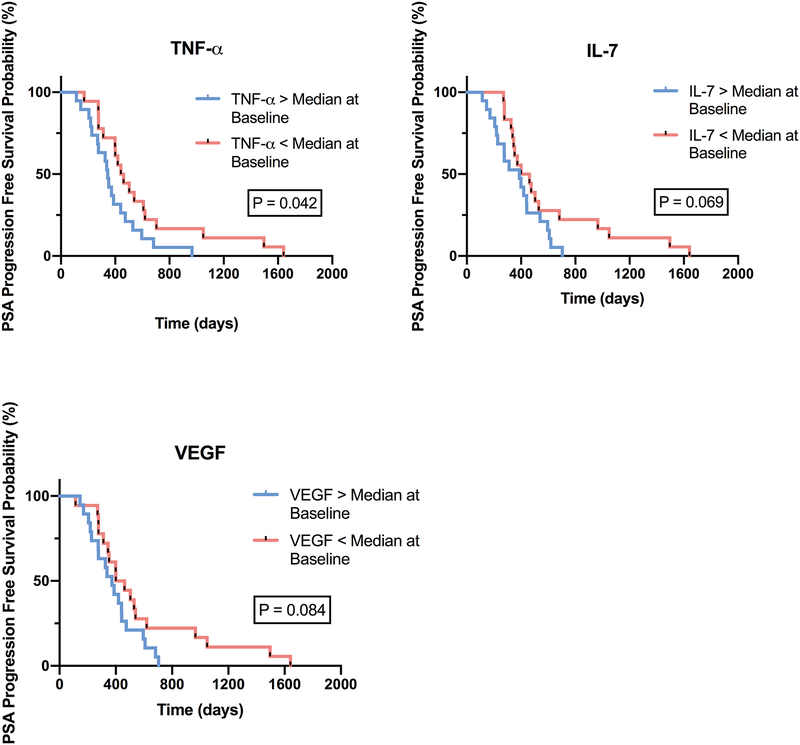
Results: Median TTPP was 399 days (range, 114-1641). Median prostate-specific antigen (PSA) at baseline and progression were 8.5 and 5.3 ng/mL, respectively. Twenty-three patients (62%) achieved undetectable PSA with ADT. Castrate levels of testosterone (<50 ng/dL) after 3 months of ADT occurred in 35 patients (95%). TNF-α (P = .002), IL-23 (P = .002), and CXCL10 (P = .001) significantly increased from baseline to post ADT. Certain cytokines correlated longitudinally: TNF-α correlated with IL-23 (r = .72; P < .001) and IL-8 (r = .59; P < .001) from baseline to post ADT and to PSA progression. Neutrophil-to-lymphocyte ratio correlated with IL-27 (r = .57; P < .001) and MIP-3α (r = .56; P < .001). Patients with a detectable PSA after ADT had elevated levels of IL-6 (P = .049) and IL-8 (P = .013) at PSA progression as compared with those with an undetectable PSA. There was a trend toward shorter TTPP in patients with TNF-α levels above the median (P = .042).
Conclusions: Several innate cytokines were associated with biochemically recurrent prostate cancer.
Keywords: IL-23; IL-8; TNF-α; biochemical recurrence.
© 2019 Wiley Periodicals, Inc.
Conflict of interest statement
Figures
References
-
- Kupelian PA, Mahadevan A, Reddy CA, Reuther AM, Klein EA. Use of different definitions of biochemical failure after external beam radiotherapy changes conclusions about relative treatment efficacy for localized prostate cancer. Urology. 2006;68(3):593–598. - PubMed
-
- Hodge DR, Hurt EM, Farrar WL. The role of IL-6 and STAT3 in inflammation and cancer. Eur J Cancer. 2005;41(16):2502–2512. - PubMed
-
- Dranoff G Cytokines in cancer pathogenesis and cancer therapy. Nat Rev Cancer. 2004;4(1):11–22. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
