

Specific motor cortex hypoexcitability and hypoactivation in COPD patients with peripheral muscle weakness
- PMID: 31900129
- PMCID: PMC6942311
- DOI: 10.1186/s12890-019-1042-0
Specific motor cortex hypoexcitability and hypoactivation in COPD patients with peripheral muscle weakness
Abstract
Background: Peripheral muscle weakness can be caused by both peripheral muscle and neural alterations. Although peripheral alterations cannot totally explain peripheral muscle weakness in COPD, the existence of an activation deficit remains controversial. The heterogeneity of muscle weakness (between 32 and 57% of COPD patients) is generally not controlled in studies and could explain this discrepancy. This study aimed to specifically compare voluntary and stimulated activation levels in COPD patients with and without muscle weakness.
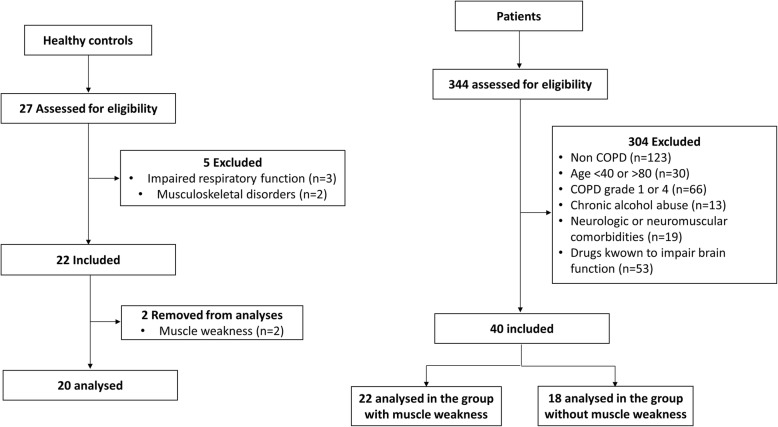
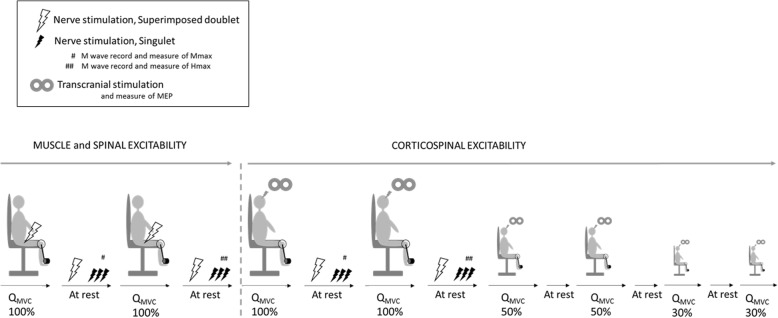
Methods: Twenty-two patients with quadriceps weakness (COPDMW), 18 patients with preserved quadriceps strength (COPDNoMW) and 20 controls were recruited. Voluntary activation was measured through peripheral nerve (VAperipheral) and transcranial magnetic (VAcortical) stimulation. Corticospinal and spinal excitability (MEP/Mmax and Hmax/Mmax) and corticospinal inhibition (silent period duration) were assessed during maximal voluntary quadriceps contractions.
Results: COPDMW exhibited lower VAcortical and lower MEP/Mmax compared with COPDNoMW (p < 0.05). Hmax/Mmax was not significantly different between groups (p = 0.25). Silent period duration was longer in the two groups of COPD patients compared with controls (p < 0.01). Interestingly, there were no significant differences between all COPD patients taken together and controls regarding VAcortical and MEP/Mmax.
Conclusions: COPD patients with muscle weakness have reduced voluntary activation without altered spinal excitability. Corticospinal inhibition is higher in COPD regardless of muscle weakness. Therefore, reduced cortical excitability and a voluntary activation deficit from the motor cortex are the most likely cortical mechanisms implicated in COPD muscle weakness. The mechanisms responsible for cortical impairment and possible therapeutic interventions need to be addressed.
Keywords: Chronic obstructive pulmonary disease; Corticospinal excitability; Motor cortex; Peripheral muscle weakness.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Locke E, Thielke S, Diehr P, Wilsdon AG, Graham Barr R, Hansel N, et al. Effects of respiratory and non-respiratory factors on disability among older adults with airway obstruction: the cardiovascular health study. COPD: J Chron Obstruct Pulmon Dis. 2013;10(5):588–596. doi: 10.3109/15412555.2013.781148. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
