

Reliability, validity and discriminant ability of a robotic device for finger training in patients with subacute stroke
- PMID: 31900169
- PMCID: PMC6942416
- DOI: 10.1186/s12984-019-0634-5
Reliability, validity and discriminant ability of a robotic device for finger training in patients with subacute stroke
Abstract
Background: The majority of stroke survivors experiences significant hand impairments, as weakness and spasticity, with a severe impact on the activity of daily living. To objectively evaluate hand deficits, quantitative measures are needed. The aim of this study is to assess the reliability, the validity and the discriminant ability of the instrumental measures provided by a robotic device for hand rehabilitation, in a sample of patients with subacute stroke.
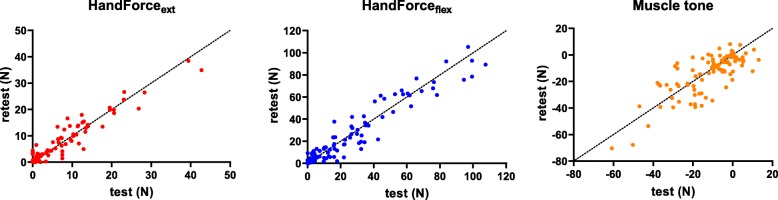
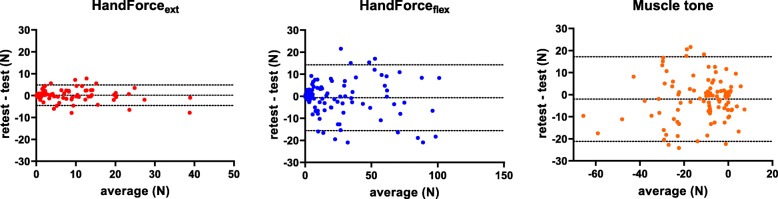
Material and methods: In this study, 120 patients with stroke and 40 controls were enrolled. Clinical evaluation included finger flexion and extension strength (using the Medical Research Council, MRC), finger spasticity (using the Modified Ashworth Scale, MAS) and motor control and dexterity during ADL performance (by means of the Frenchay Arm Test, FAT). Robotic evaluations included finger flexion and extension strength, muscle tone at rest, and instrumented MAS and Modified Tardieu Scale. Subjects were evaluated twice, one day apart, to assess the test-retest reliability of the robotic measures, using the Intraclass Correlation Coefficient (ICC). To estimate the response stability, the standard errors of measurement and the minimum detectable change (MDC) were also calculated. Validity was assessed by analyzing the correlations between the robotic metrics and the clinical scales, using the Spearman's Correlation Coefficient (r). Finally, we investigated the ability of the robotic measures to distinguish between patients with stroke and healthy subjects, by means of Mann-Whitney U tests.
Results: All the investigated measures were able to discriminate patients with stroke from healthy subjects (p < 0.001). Test-retest reliability was found to be excellent for finger strength (in both flexion and extension) and muscle tone, with ICCs higher than 0.9. MDCs were equal to 10.6 N for finger flexion, 3.4 N for finger extension, and 14.3 N for muscle tone. Conversely, test-retest reliability of the spasticity measures was poor. Finally, finger strength (in both flexion and extension) was correlated with the clinical scales (r of about 0.7 with MRC, and about 0.5 with FAT).
Discussion: Finger strength (in both flexion and extension) and muscle tone, as provided by a robotic device for hand rehabilitation, are reliable and sensitive measures. Moreover, finger strength is strongly correlated with clinical scales. Changes higher than the obtained MDC in these robotic measures could be considered as clinically relevant and used to assess the effect of a rehabilitation treatment in patients with subacute stroke.
Keywords: Discriminant ability; Hand; Rehabilitation; Reliability; Robotics; Stroke; Upper extremity; Validity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
