

Pediatric trauma venous thromboembolism prediction algorithm outperforms current anticoagulation prophylaxis guidelines: a pilot study
- PMID: 31900592
- PMCID: PMC7223182
- DOI: 10.1007/s00383-019-04613-y
Pediatric trauma venous thromboembolism prediction algorithm outperforms current anticoagulation prophylaxis guidelines: a pilot study
Abstract
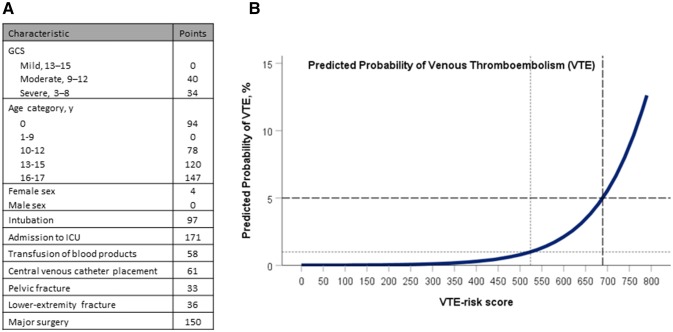
Purpose: Venous thromboembolism (VTE) in injured children is rare, but sequelae can be morbid and life-threatening. Recent trauma society guidelines suggesting that all children over 15 years old should receive thromboprophylaxis may result in overtreatment. We sought to evaluate the efficacy of a previously published VTE prediction algorithm and compare it to current recommendations.
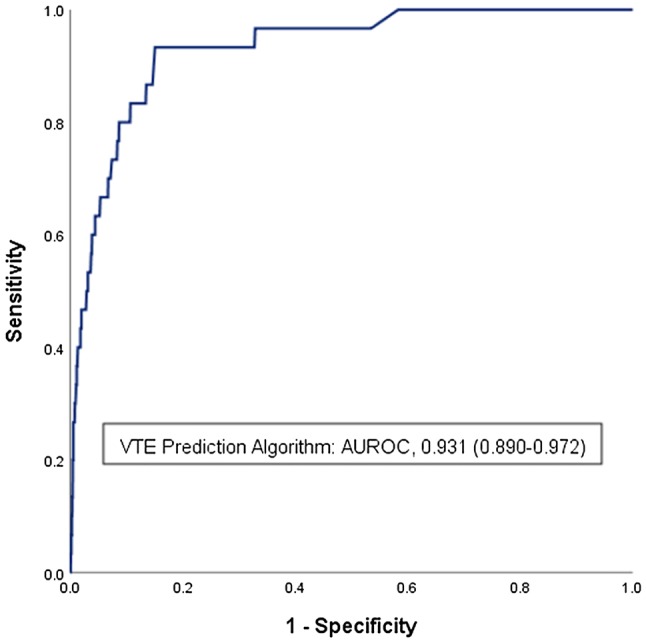
Methods: Two institutional trauma registries were queried for all pediatric (age < 18 years) patients admitted from 2007 to 2018. Clinical data were applied to the algorithm and the area under the receiver operating characteristic (AUROC) curve was calculated to test algorithm efficacy.
Results: A retrospective review identified 8271 patients with 30 episodes of VTE (0.36%). The VTE prediction algorithm classified 51 (0.6%) as high risk (> 5% risk), 322 (3.9%) as moderate risk (1-5% risk) and 7898 (95.5%) as low risk (< 1% risk). AUROC was 0.93 (95% CI 0.89-0.97). In our population, prophylaxis of the 'moderate-' and 'high-risk' cohorts would outperform the sensitivity (60% vs. 53%) and specificity (96% vs. 77%) of current guidelines while anticoagulating substantially fewer patients (373 vs. 1935, p < 0.001).
Conclusion: A VTE prediction algorithm using clinical variables can identify injured children at risk for venous thromboembolic disease with more discrimination than current guidelines. Prospective studies are needed to investigate the validity of this model.
Level of evidence: III-Clinical decision rule evaluated in a single population.
Keywords: Guidelines; Pediatric trauma; Thromboprophylaxis; Venous thromboembolism.
Conflict of interest statement
The following authors AC, ED, SL, KH, EB, CC, LM, KD, NH, SK, MS, MJ have no financial disclosures.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
