

Enhanced Recovery After Surgery (ERAS) Reduces Hospital Costs and Improve Clinical Outcomes in Liver Surgery: a Systematic Review and Meta-Analysis
- PMID: 31900738
- PMCID: PMC7165160
- DOI: 10.1007/s11605-019-04499-0
Enhanced Recovery After Surgery (ERAS) Reduces Hospital Costs and Improve Clinical Outcomes in Liver Surgery: a Systematic Review and Meta-Analysis
Abstract
Background: Enhanced recovery after surgery (ERAS) protocols are evidence-based, multimodal and patient-centred approach to optimize patient care and experience during their perioperative pathway. It has been shown to be effective in reducing length of hospital stay and improving clinical outcomes. However, evidence on its effective in liver surgery remains weak. The aim of this review is to investigate clinical benefits, cost-effectiveness and compliance to ERAS protocols in liver surgery.
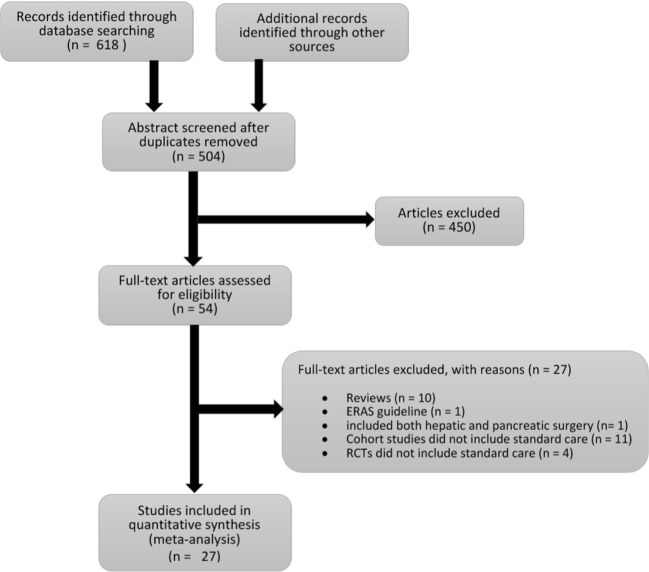
Methods: A systematic literature search was conducted using CINAHL Plus, EMBASE, MEDLINE, PubMed and Cochrane for randomized control trials (RCTs) and cohort studies published between 2008 and 2019, comparing effect of ERAS protocols and standard care on hospital cost, LOS, complications, readmission, mortality and compliance.
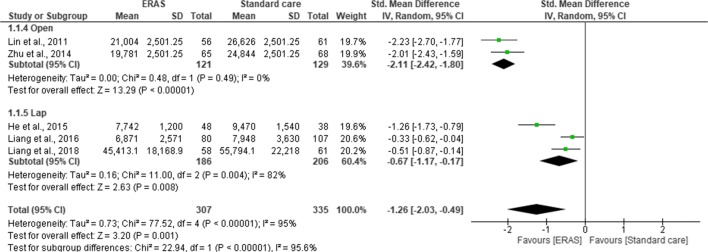
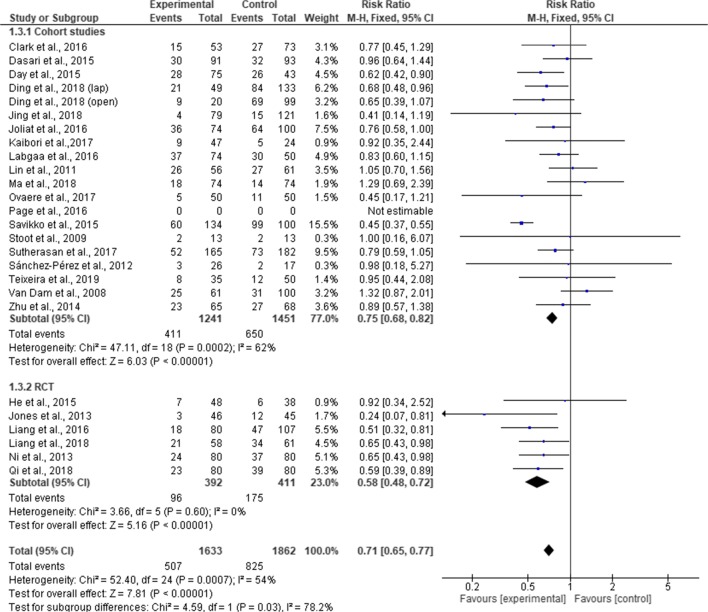
Results: The search resulted in 6 RCTs and 21 cohort studies of 3739 patients (1777 in ERAS and 1962 in standard care group). LOS was reduced by 2.22 days in ERAS group (MD = -2.22; CI, -2.77 to -1.68; p < 0.00001) compared to the standard care group. Fewer patients in ERAS group experienced complications (RR, 0.71; 95% CI, 0.65-0.77; p = < 0.00001). Hospital cost was significantly lower in the ERAS group (SMD = -0.98; CI, -1.37 to - 0.58; p < 0.0001).
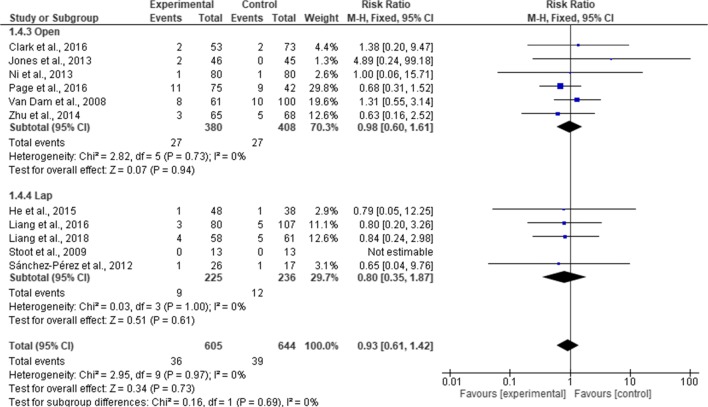
Conclusion: Our review concluded that the introduction of ERAS protocols is safe and feasible in hepatectomies, without increasing mortality and readmission rates, whilst reducing LOS and risk of complications, and with a significant hospital cost savings. Laparoscopic approach may be necessary to reduce complication rates in liver surgery. However, further studies are needed to investigate overall compliance to ERAS protocols and its impact on clinical outcomes.
Keywords: Enhanced recovery after surgery; Liver surgery; Systematic review and meta-analysis.
Figures







References
-
- Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–17. - PubMed
-
- van Dam RM, et al. Initial experience with a multimodal enhanced recovery programme in patients undergoing liver resection. Br J Surg. 2008;95(8):969–75. - PubMed
-
- MacKay G, O'Dwyer PJ. Early discharge following liver resection for colorectal metastases. Scott Med J. 2008;53(2):22–4. - PubMed
-
- Melloul E, et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J Surg. 2016;40(10):2425–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
