

Time-varying pattern of recurrence risk for localized melanoma in China
- PMID: 31901239
- PMCID: PMC6942369
- DOI: 10.1186/s12957-019-1775-5
Time-varying pattern of recurrence risk for localized melanoma in China
Abstract
Background: Acral and mucosal melanomas are rarely seen in Caucasians but common in China. There are limited data on the recurrence characteristics for these patients. This study aimed to identify the recurrence pattern for localized melanoma in China, especially acral and mucosal subtypes.
Methods: Patients with localized melanoma who underwent radical resection between January 1999 and December 2014 in southern China were retrospectively reviewed. Survival and annual recurrence hazard were analyzed by Kaplan-Meier method and hazard function, respectively.
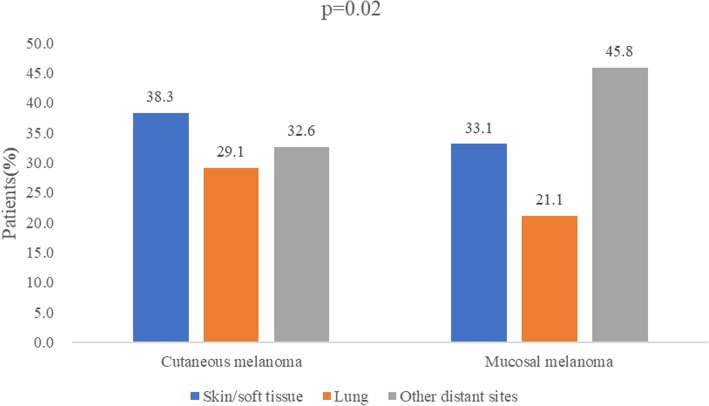
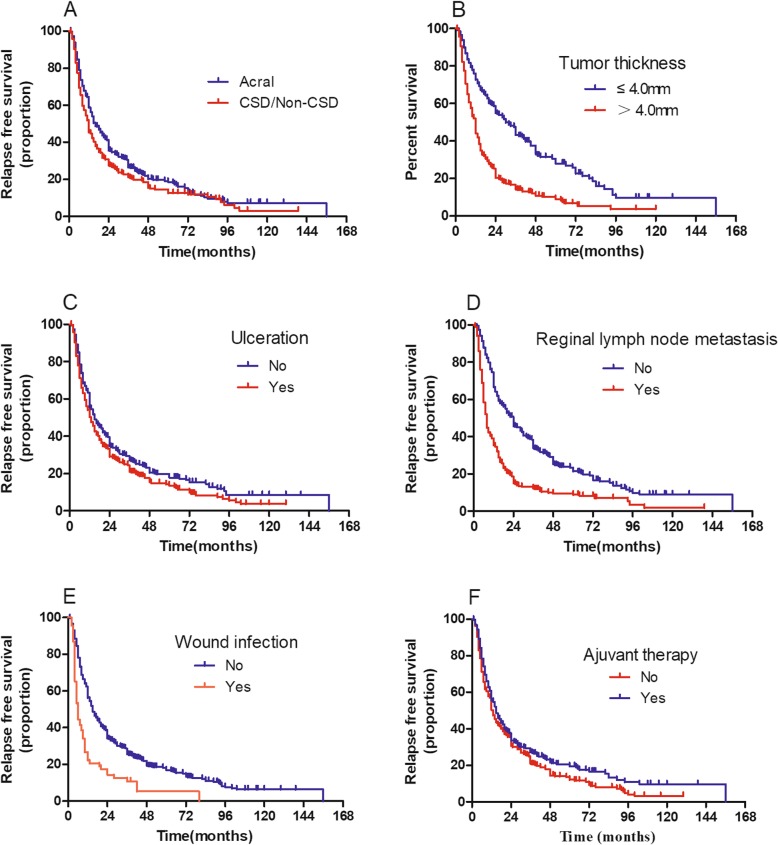
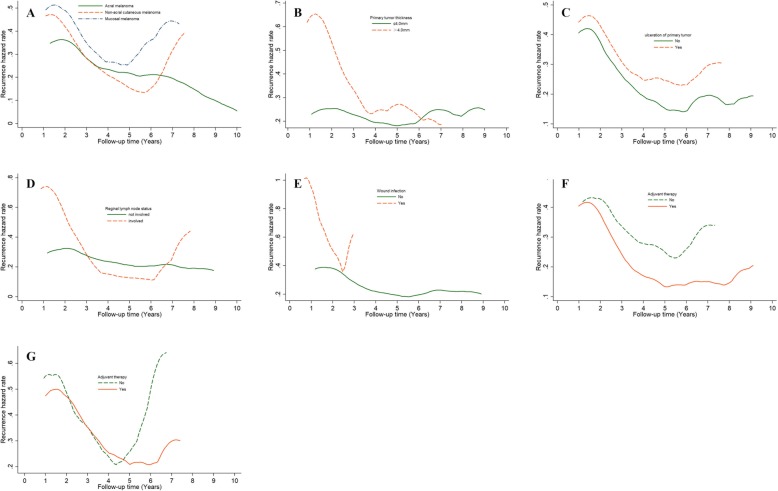
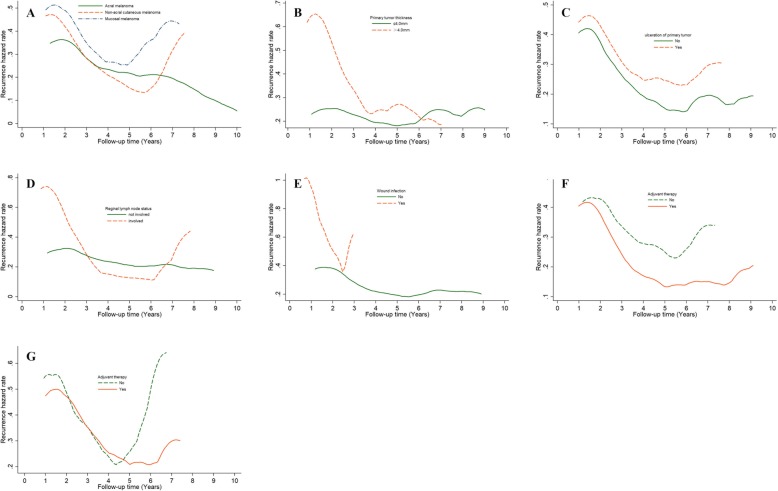
Results: Totally, 1012 patients were included (acral melanoma 400; chronic sun-induced damage (CSD)/non-CSD melanoma 314; mucosal melanoma 298). Recurrence was recorded in 808 patients (localized 14.1%; regional 29.6%, and distant 56.3%). Mucosal melanoma had local and M1c stage recurrence more frequently than cutaneous melanoma, but less frequent regional node relapse. There was no difference in recurrent site distribution between acral and CSD/non-CSD melanoma. The annual recurrence hazard curve for the entire cohort showed a double-peaked pattern with the first major peak in the second year after surgery and the second peak near the seventh year. Mucosal melanoma had a higher recurrence risk than cutaneous melanoma. Acral melanoma had a lower flat recurrence peak than CSD/non-CSD melanoma. Tumor thickness > 4.0 mm, ulceration, positive regional nodes, and wound infection were associated with a higher recurrence risk in cutaneous melanoma. Adjuvant therapy reduced the recurrence risk of cutaneous melanoma but not of mucosal melanoma.
Conclusions: This is a large cohort about the rule of recurrence risk in acral and mucosal melanoma and will provide an initial framework for development of surveillance and adjuvant strategy for Chinese melanoma patients.
Keywords: Chinese population; Melanoma; Recurrence hazard.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Pattern and incidence of first site recurrences following sentinel node procedure in melanoma patients.World J Surg. 2002 Dec;26(12):1405-11. doi: 10.1007/s00268-002-6197-8. Epub 2002 Sep 26. World J Surg. 2002. PMID: 12297910
-
Patterns of initial recurrence and prognosis after sentinel lymph node biopsy and selective lymphadenectomy for melanoma.Plast Reconstr Surg. 2003 Aug;112(2):486-97. doi: 10.1097/01.PRS.0000070989.23469.1F. Plast Reconstr Surg. 2003. PMID: 12900606
-
[Descriptive analysis of cutaneous recurrence patterns in patients with melanoma].Actas Dermosifiliogr. 2011 Dec;102(10):791-6. doi: 10.1016/j.ad.2011.04.006. Epub 2011 Jun 11. Actas Dermosifiliogr. 2011. PMID: 21658662 Spanish.
-
The 2018 World Health Organization Classification of Cutaneous, Mucosal, and Uveal Melanoma: Detailed Analysis of 9 Distinct Subtypes Defined by Their Evolutionary Pathway.Arch Pathol Lab Med. 2020 Apr;144(4):500-522. doi: 10.5858/arpa.2019-0561-RA. Epub 2020 Feb 14. Arch Pathol Lab Med. 2020. PMID: 32057276 Review.
-
Immunotherapy in Acral and Mucosal Melanoma: Current Status and Future Directions.Front Immunol. 2021 Jun 4;12:680407. doi: 10.3389/fimmu.2021.680407. eCollection 2021. Front Immunol. 2021. PMID: 34149718 Free PMC article. Review.
Cited by
-
Living photosynthetic microneedle patches for in situ oxygenation and postsurgical melanoma therapy.J Nanobiotechnology. 2024 Nov 11;22(1):698. doi: 10.1186/s12951-024-02982-8. J Nanobiotechnology. 2024. PMID: 39529107 Free PMC article.
-
BRAF and NRAS Mutations and the Association with Prognosis of Acral Lentiginous and Nodular Melanomas in Indonesia.Asian Pac J Cancer Prev. 2024 Oct 1;25(10):3525-3531. doi: 10.31557/APJCP.2024.25.10.3525. Asian Pac J Cancer Prev. 2024. PMID: 39471018 Free PMC article.
-
Endoscopic ultrasound features of rectal melanoma: A case report and review of literature.World J Clin Cases. 2024 Jun 6;12(16):2862-2868. doi: 10.12998/wjcc.v12.i16.2862. World J Clin Cases. 2024. PMID: 38899292 Free PMC article.
-
Immune-related gene signature associates with immune landscape and predicts prognosis accurately in patients with skin cutaneous melanoma.Front Genet. 2023 Jan 4;13:1095867. doi: 10.3389/fgene.2022.1095867. eCollection 2022. Front Genet. 2023. PMID: 36685954 Free PMC article.
-
Regional lymph node infiltration and thick lesions are associated with poor prognosis in high-risk resected melanomas: A retrospective cohort study.Ann Med Surg (Lond). 2020 Dec 16;61:132-138. doi: 10.1016/j.amsu.2020.12.004. eCollection 2021 Jan. Ann Med Surg (Lond). 2020. PMID: 33456772 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
