

Incidence of supraventricular tachycardia after inhaled short-acting beta agonist treatment in children
- PMID: 31902263
- PMCID: PMC8657863
- DOI: 10.1080/02770903.2019.1709867
Incidence of supraventricular tachycardia after inhaled short-acting beta agonist treatment in children
Abstract
Introduction: Albuterol can trigger supraventricular tachycardia (SVT). The clinical characteristics, incidence, and risk factors of SVT after inhaled SABA treatment in children are currently unknown. Through review of regional care delivery, we will describe cases of SVT during asthma treatment in hospital-based settings, define the incidence of SVT in our population, and evaluate risk factors of SABA-induced SVT.
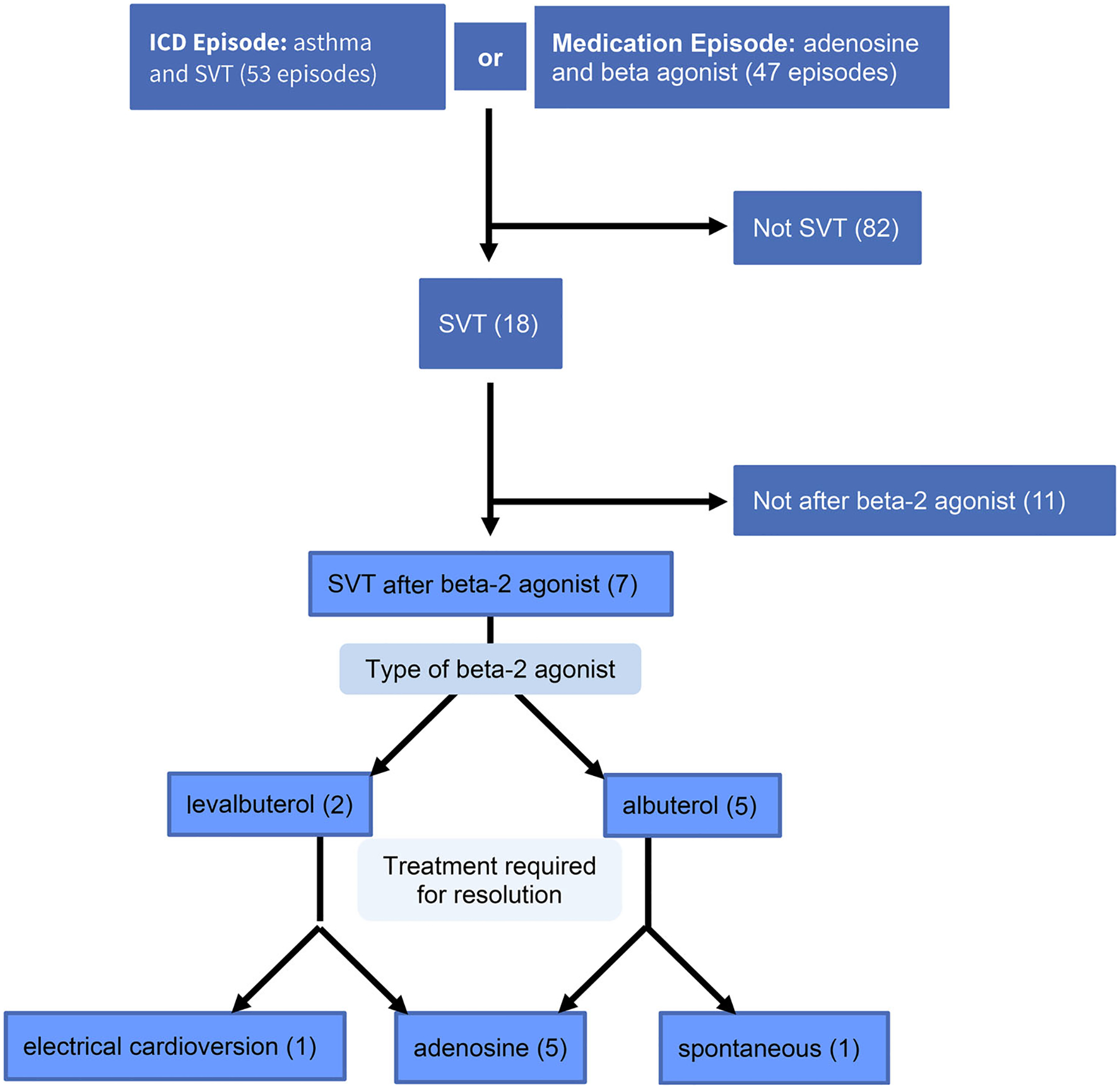
Methods: We identified hospital-based care episodes of children 0-18 years old between 2006 and 2015 recorded in the Intermountain Healthcare EDW with either 1) diagnosis codes for both asthma and SVT or 2) both SABA and adenosine listed as billed medications. Controls were matched with cases by age and sex to determine risk factors for SVT after SABA using conditional logistic regression.
Results: Of 93 care episodes meeting criteria, we found 7 cases of SVT after SABA treatment in 6 patients over 10 years. In our population, the incidence of SVT is 3.9 per 10,000 episodes of SABA treatment, and 5.1 per 10,000 children with asthma receiving hospital-based asthma care. Two episodes of SVT followed treatment with only levalbuterol, three after only albuterol, and two after both albuterol and levalbuterol treatment. Five cases of SVT were converted to sinus rhythm with adenosine, one converted with synchronized electrical cardioversion, and one resolved spontaneously. No cases of SVT led to death. No examined variables were associated with SABA-induced SVT.
Conclusions: SVT is rare during hospital-based treatment for acute asthma using inhaled SABAs and has low morbidity and mortality.
Keywords: Case reports; control/management.
Conflict of interest statement
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
-
- Roemer M. Health care expenditures for the five most common children’s conditions, 2008: estimates for U.S. Civilian Noninstitutionalized Children, Ages 0–17; Agency for Healthcare Research and Quality; 2011.
-
- National Asthma Education and Prevention Program. Guidelines for the diagnosis and management of asthma. Bethesda, MD: National Heart Lung and Blood Institue, National Institutes of Health, U.S. Department of Health and Human Services; 2007.
-
- Bozzola E, Bozzola M, Barberi S, Cutrera R, Villani A. Safety and potential side effects of beta 2-agonists: a still debated question. Int J Pediatr Child Health. 2013;1(1):4–10. doi: 10.12974/2311-8687.2013.01.01.2. - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical