

Therapeutic options for mucinous ovarian carcinoma
- PMID: 31902686
- PMCID: PMC7056511
- DOI: 10.1016/j.ygyno.2019.12.015
Therapeutic options for mucinous ovarian carcinoma
Abstract
Objective: Mucinous ovarian carcinoma (MOC) is an uncommon ovarian cancer histotype that responds poorly to conventional chemotherapy regimens. Although long overall survival outcomes can occur with early detection and optimal surgical resection, recurrent and advanced disease are associated with extremely poor survival. There are no current guidelines specifically for the systemic management of recurrent MOC. We analyzed data from a large cohort of women with MOC to evaluate the potential for clinical utility from a range of systemic agents.
Methods: We analyzed gene copy number (n = 191) and DNA sequencing data (n = 184) from primary MOC to evaluate signatures of mismatch repair deficiency and homologous recombination deficiency, and other genetic events. Immunohistochemistry data were collated for ER, CK7, CK20, CDX2, HER2, PAX8 and p16 (n = 117-166).
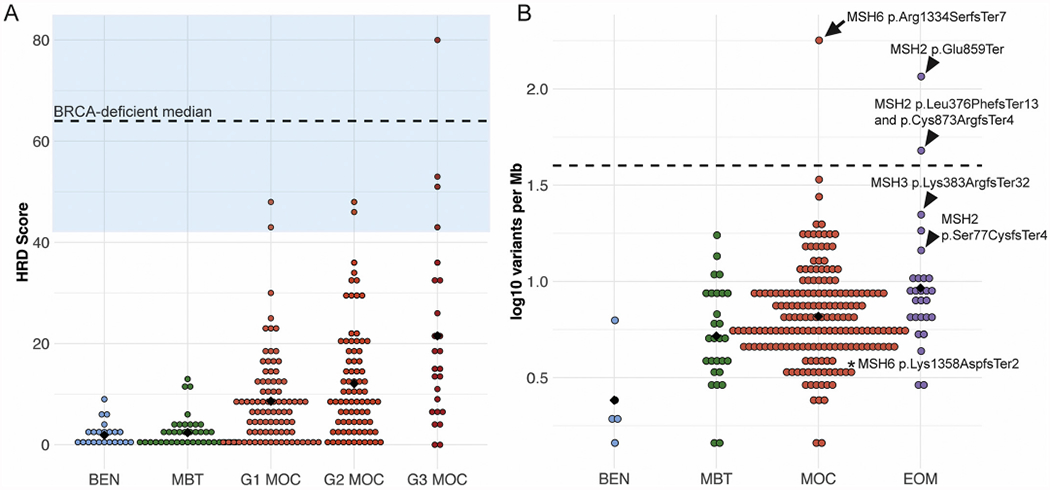
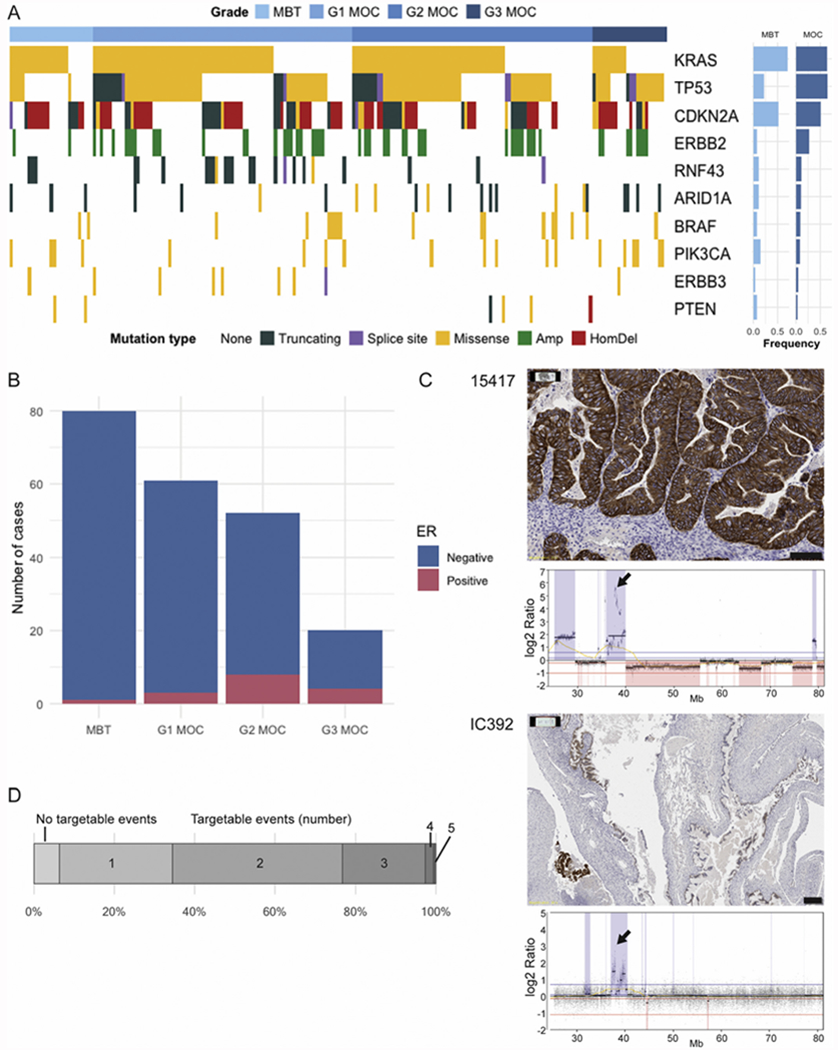
Results: Molecular aberrations noted in MOC that suggest a match with current targeted therapies include amplification of ERBB2 (26.7%) and BRAF mutation (9%). Observed genetic events that suggest potential efficacy for agents currently in clinical trials include: KRAS/NRAS mutations (66%), TP53 missense mutation (49%), RNF43 mutation (11%), ARID1A mutation (10%), and PIK3CA/PTEN mutation (9%). Therapies exploiting homologous recombination deficiency (HRD) may not be effective in MOC, as only 1/191 had a high HRD score. Mismatch repair deficiency was similarly rare (1/184).
Conclusions: Although genetically diverse, MOC has several potential therapeutic targets. Importantly, the lack of response to platinum-based therapy observed clinically corresponds to the lack of a genomic signature associated with HRD, and MOC are thus also unlikely to respond to PARP inhibition.
Keywords: Genomic; Molecular targeted therapy; Ovarian cancer; Precision oncology; Sequencing; Therapy.
Copyright © 2019 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare no conflicts of interest. ADF, NT and DDLB have received research grant funding from AstraZeneca, unrelated to the contents on this manuscript. DDLB also reports funding from Roche-Genentech and BeiGene, also unrelated. CG reports funding from AstraZeneca, Roche, Clovis, Tesaro, Foundation One, Nucana, Aprea, Novartis, Chugai, and MSD, all outside the submitted work. CLS reports non-financial support and/or other support from Clovis Oncology, Roche, Eisai Australia, Beigene, Sierra Oncology, and AstraZeneca, all outside the submitted work.
Figures

References
-
- Shimada M, Kigawa J, Ohishi Y, et al. , Clinicopathological characteristics of mucinous adenocarcinoma of the ovary, Gynecol. Oncol. 113 (3) (2009) 331–334. - PubMed
-
- Bamias A, Sotiropoulou M, Zagouri F, et al. , Prognostic evaluation of tumour type and other histopathological characteristics in advanced epithelial ovarian cancer, treated with surgery and paclitaxel/carboplatin chemotherapy: cell type is the most useful prognostic factor, Eur. J. Cancer 48 (10) (2011) 1476–1483. - PubMed
-
- Mackay HJ, Brady MF, Oza AM, et al. , Prognostic relevance of uncommon ovarian histology inwomen with stage III/IV epithelial ovarian cancer, Int. J. Gynecol. Cancer 20 (6) (2010) 945–952. - PubMed
-
- Gore M, Hackshaw A,Brady WE, et al. , An international, phase III randomized trial in patients with mucinous epithelial ovarian cancer (mEOC/GOG 0241) with longterm follow-up: and experience of conducting a clinical trial in a rare gynecological tumor, Gynecol. Oncol. 153 (3) (2019) 541–548. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
