

Algorithm-based troubleshooting to manage bleeding during thoracoscopic anatomic pulmonary resection
- PMID: 31903243
- PMCID: PMC6940248
- DOI: 10.21037/jtd.2019.10.72
Algorithm-based troubleshooting to manage bleeding during thoracoscopic anatomic pulmonary resection
Abstract
Background: Few studies have reported on the effects of intraoperative complications, such as vessel injury, during thoracoscopic anatomic pulmonary resection. We evaluated intraoperative vessel injury and assessed troubleshooting methods for thoracoscopic anatomic pulmonary resection.
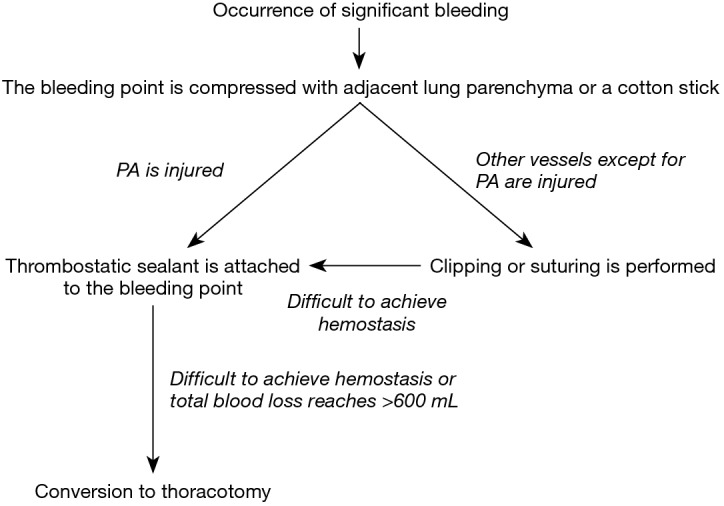
Methods: A total of 378 patients underwent thoracoscopic anatomic pulmonary resection between April 2012 and March 2018, 40 of whom were identified as having an intraoperative vessel injury. In our department, we treat significant bleeding based on the algorithm shown in Figure 1. We analyzed the injured vessels and hemostatic procedures employed and compared perioperative outcomes in patients with (n=40) or without (n=338) a vessel injury. Additionally, we examined the data on a year-by-year basis from April 2012, and perioperative results were compared in each year.
Results: The vessel injured was a branch of the pulmonary artery in 22 cases (55%). Hemostasis was achieved by applying a thrombostatic sealant in 26 cases (65%). Although patients without a vessel injury had a shorter operation time, less intraoperative blood loss, and shorter duration of chest tube drainage, no significant differences in the length of postoperative hospitalization or morbidity were observed. The occurrence rate of significant intraoperative bleeding in the last year measured was similar to that in the first year measured.
Conclusions: Thoracoscopic anatomic pulmonary resection is feasible and safe if the surgeon performs appropriate hemostasis, although vascular hazards might be inherent during thoracoscopic anatomic pulmonary resection, regardless of the surgeon's experience.
Keywords: Algorithm; intraoperative bleeding; pulmonary resection; thoracoscopy; troubleshooting.
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Meeting presentation: the abstract was presented at the Clinical/Outcomes, Cardiothoracic and Vascular QuickShot Session, American Surgical Congress, Houston, TX, USA, on 7 February 2019.
Figures
Comment in
-
How to reduce bleeding complications during thoracoscopic anatomic pulmonary resection.J Thorac Dis. 2020 May;12(5):1758-1761. doi: 10.21037/jtd-20-1624. J Thorac Dis. 2020. PMID: 32642079 Free PMC article. No abstract available.
References
-
- Stephens N, Rice D, Correa A, et al. Thoracoscopic lobectomy is associated with improved short-term and equivalent oncological outcomes compared with open lobectomy for clinical Stage I non-small cell lung cancer: a propensity-matched analysis of 963 cases. Eur J Cardiothorac Surg 2014;46:607-13. 10.1093/ejcts/ezu036 - DOI - PubMed
-
- Jeon JH, Kang CH, Kim HS, et al. Video-assisted thoracoscopic lobectomy in non-small-cell lung cancer patients with chronic obstructive pulmonary disease is associated with lower pulmonary complications than open lobectomy: a propensity score-matched analysis. Eur J Cardiothorac Surg 2014;45:640-5. 10.1093/ejcts/ezt460 - DOI - PubMed
-
- Scott WJ, Allen MS, Darling G, et al. Video-assisted thoracic surgery versus open lobectomy for lung cancer: A secondary analysis of data from the American College of Surgeons Oncology Group Z0030 randomised clinical trial. J Thorac Cardiovasc Surg 2010;139:976-81. 10.1016/j.jtcvs.2009.11.059 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous