

Higher Acuity Resource Utilization With Older Age and Poorer HIV Control in Adolescents and Young Adults in the HIV Research Network
- PMID: 31904706
- PMCID: PMC7055514
- DOI: 10.1097/QAI.0000000000002280
Higher Acuity Resource Utilization With Older Age and Poorer HIV Control in Adolescents and Young Adults in the HIV Research Network
Abstract
Background: Adolescents and young adults (AYA) with HIV experience poorer health outcomes compared with adults. To improve care for AYA with HIV, information about patterns of costly health care resource utilization is needed.
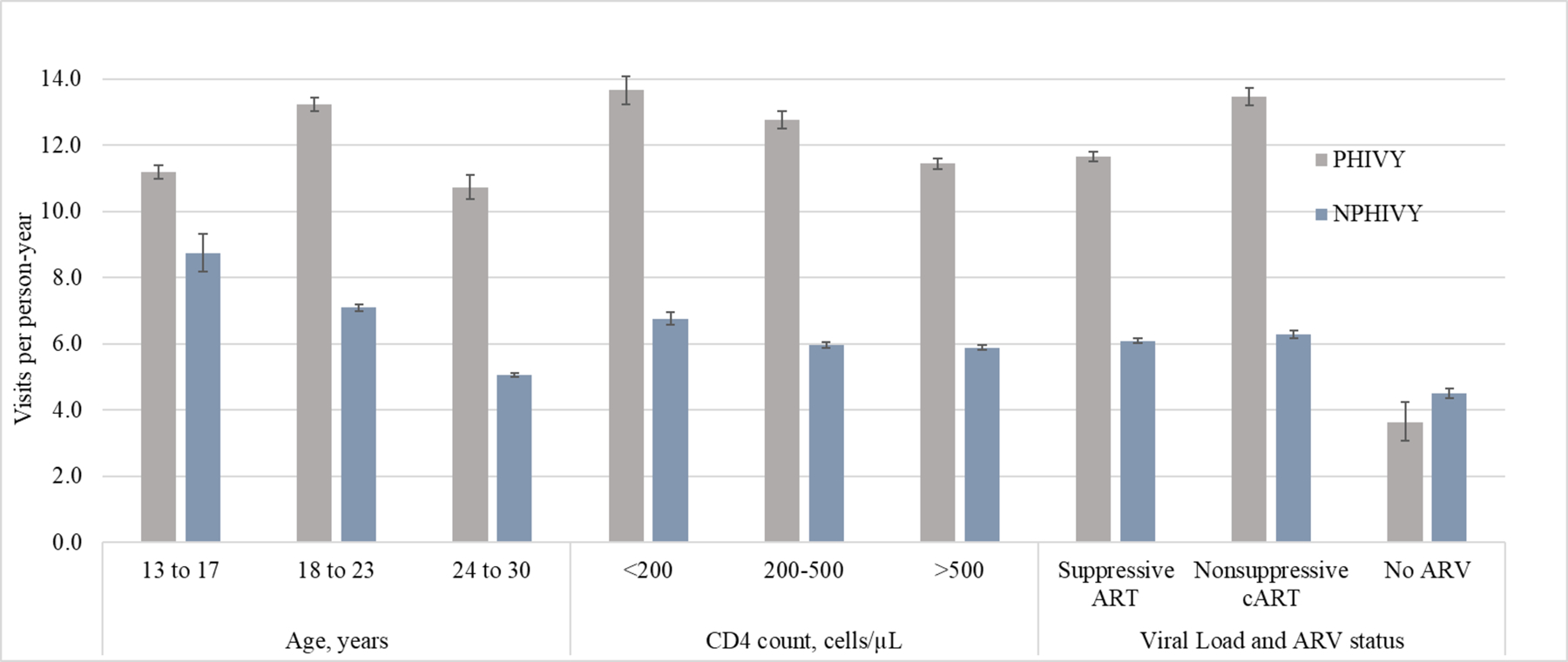
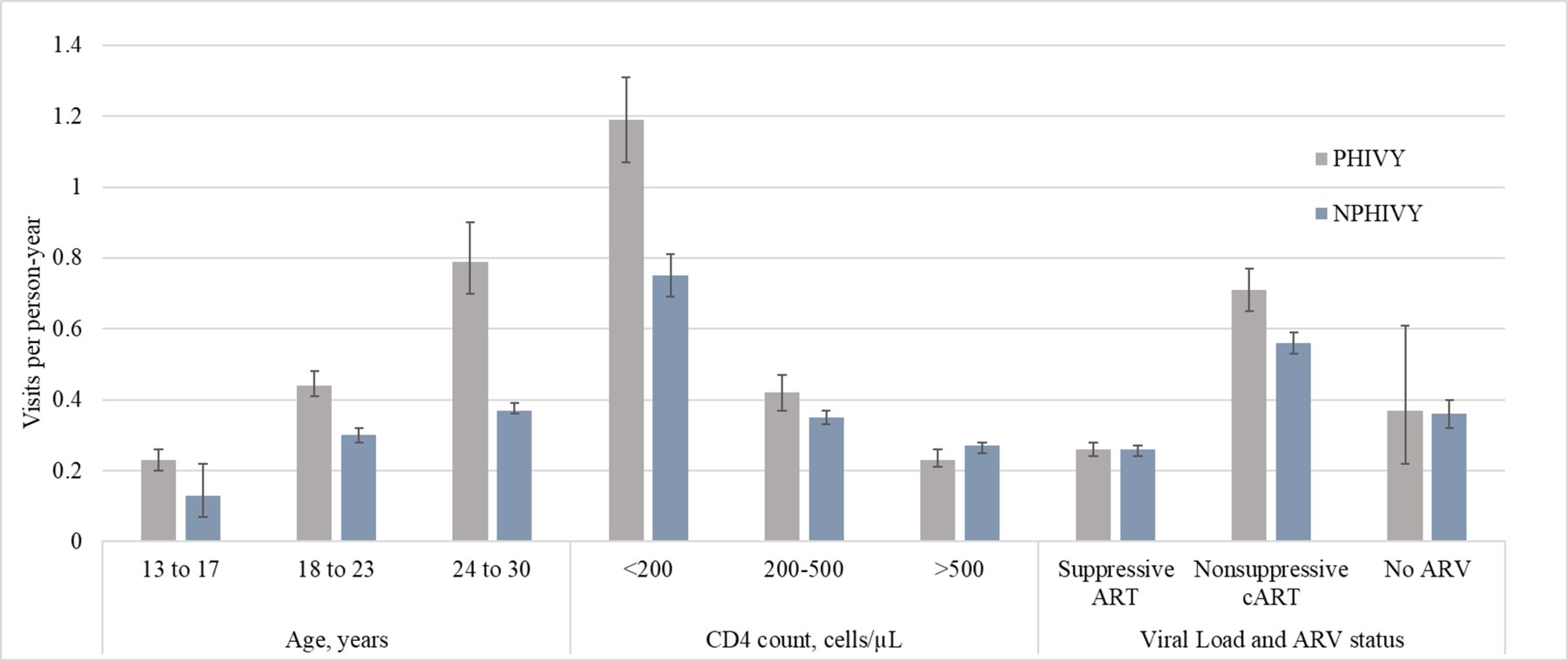
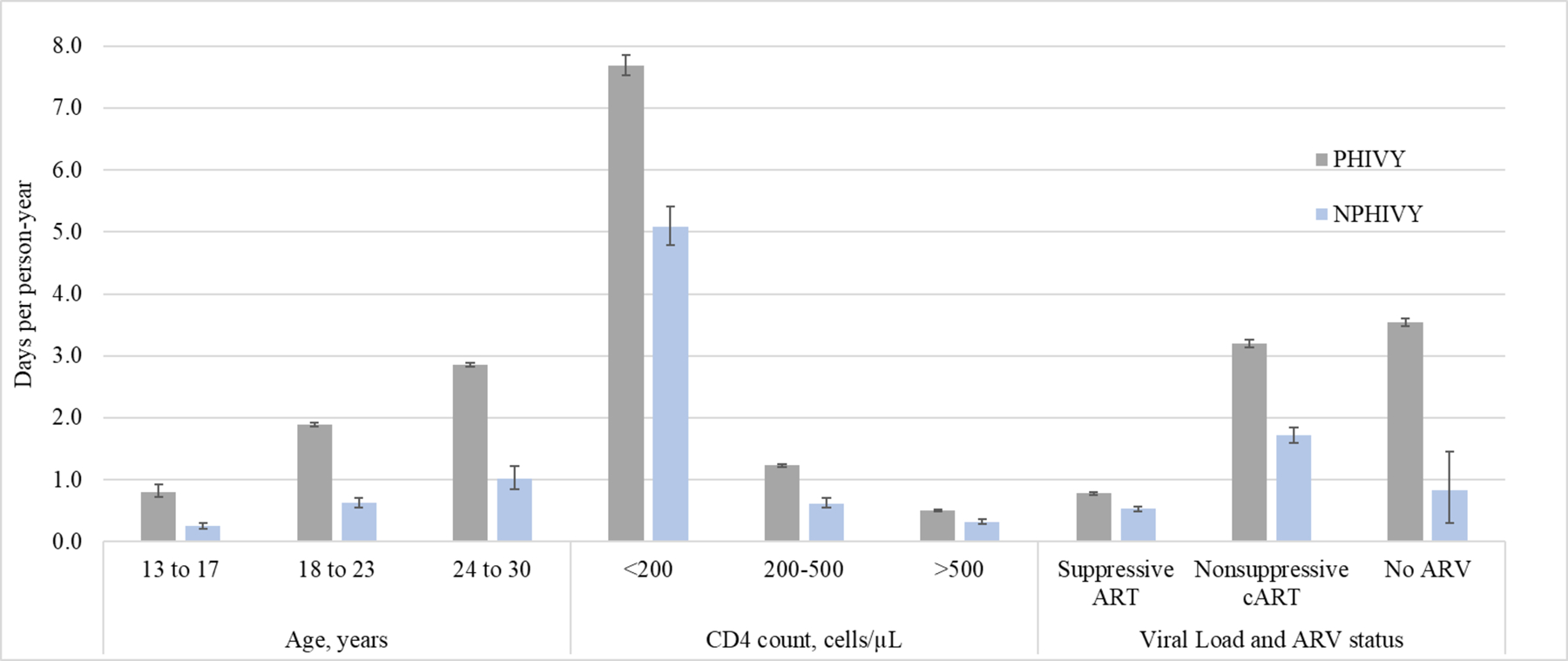
Methods: Among 13-30 year olds in the US HIV Research Network, we stratified outpatient visits, emergency department (ED) visits, and inpatient days/person-year (PY) by HIV acquisition model [perinatal (PHIVY) and nonperinatal (NPHIVY)], age (13-17, 18-23, and 24-30 years), CD4 strata (<200, 200-499, and ≥500 cells/µL), and viral load (VL) suppression (<, ≥400 copies/mL [c/mL]) combined with antiretroviral (ARV) use.
Results: Among 4540 AYA (PHIVY: 15%; NPHIVY: 85%), mean follow-up was 2.8 years. Among PHIVY, most person-time (PT) was spent between ages 13 and 23 years (13-17 years: 43%; 18-23 years: 45%), CD4 ≥500/µL (61%), and VL <400 c/mL (69%). Among NPHIVY, most PT was spent between ages 24 and 30 years (56%), with CD4 ≥500/µL (54%), and with VL <400 c/mL (67%). PT spent while prescribed ARVs and with VL ≥400 c/mL was 29% (PHIVY) and 24% (NPHIVY). For PHIVY and NPHIVY, outpatient visit rates were higher at younger ages (13-17 years and 18-23 years), lower CD4 (<200 and 200-499/µL), and among those prescribed ARVs. Rates of ED visits and inpatient days were higher during PT spent at older ages (18-23 years and 24-30 years), lower CD4 (<200 and 200-499/µL), and VL ≥400 c/mL. Utilization was higher among PHIVY than NPHIVY (outpatient: 12.1 vs. 6.0/PY; ED: 0.4 vs. 0.3/PY; inpatient: 1.5 vs. 0.8/PY).
Conclusions: More ED visits and inpatient days were observed during time spent at older ages, lower CD4 count, and VL ≥400 c/mL. Interventions to improve virologic suppression and immune response may improve outcomes, and thus decrease costly resource utilization, for AYA with HIV.
Conflict of interest statement
Competing interests
The authors have no conflicts of interest or financial disclosures.
Figures

References
-
- Centers for Disease Control and Prevention. HIV Surveillance Report, 2014; vol.26 http://www.cdc.gov/hiv/library/reports/surveillance/. Published November 2015. Accessed November 13, 2019.
-
- Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data - United States and 6 dependent areas, 2014. HIV Surveillance Supplemental Report 2016;21(No. 4). http://www.cdc.gov/hiv/library/reports/surveillance/. Published July 2016. Accessed November 13, 2019.
-
- Hall HI, Frazier EL, Rhodes P, et al. Differences in HIV care and treatment among subpopulations in the United States. JAMA Intern Med. Jul 22 2013;173(14):1337–1344. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
