

HbA1c Levels in Type 1 Diabetes from Early Childhood to Older Adults: A Deeper Dive into the Influence of Technology and Socioeconomic Status on HbA1c in the T1D Exchange Clinic Registry Findings
- PMID: 31905008
- PMCID: PMC7640747
- DOI: 10.1089/dia.2019.0393
HbA1c Levels in Type 1 Diabetes from Early Childhood to Older Adults: A Deeper Dive into the Influence of Technology and Socioeconomic Status on HbA1c in the T1D Exchange Clinic Registry Findings
Abstract
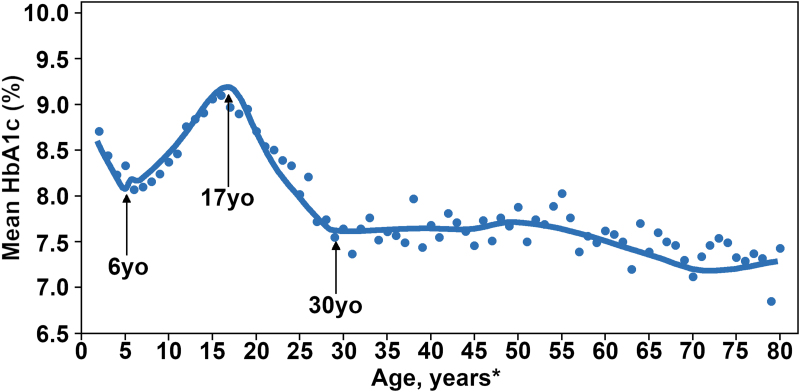
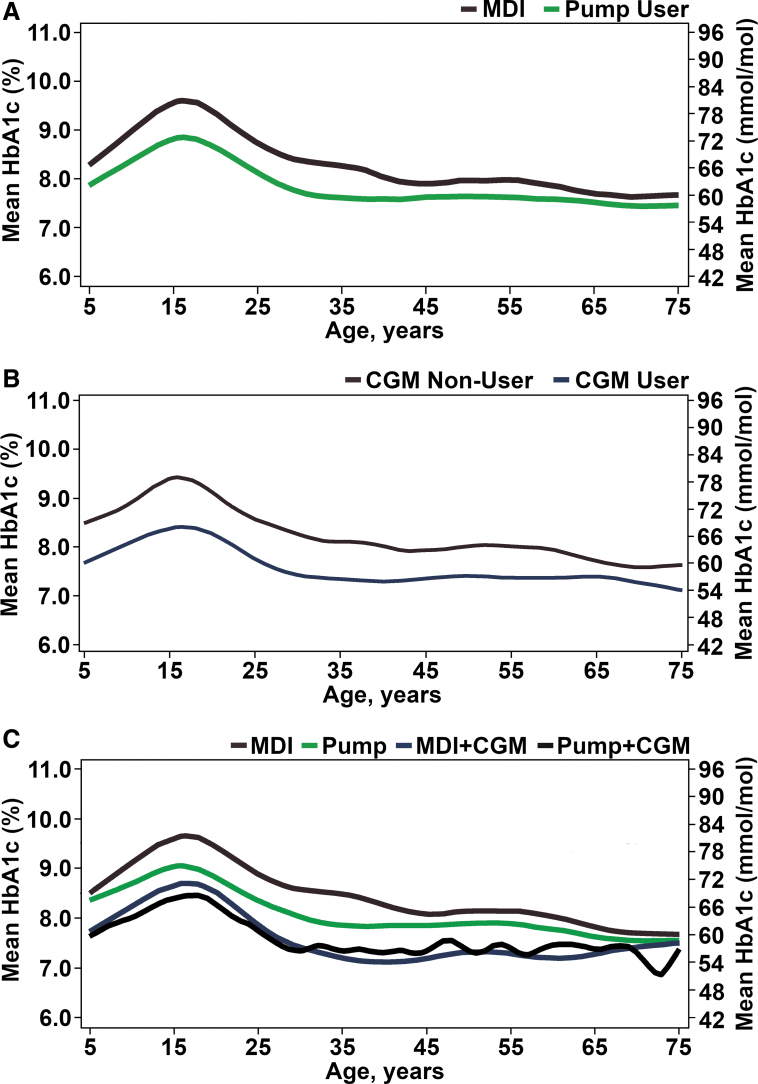
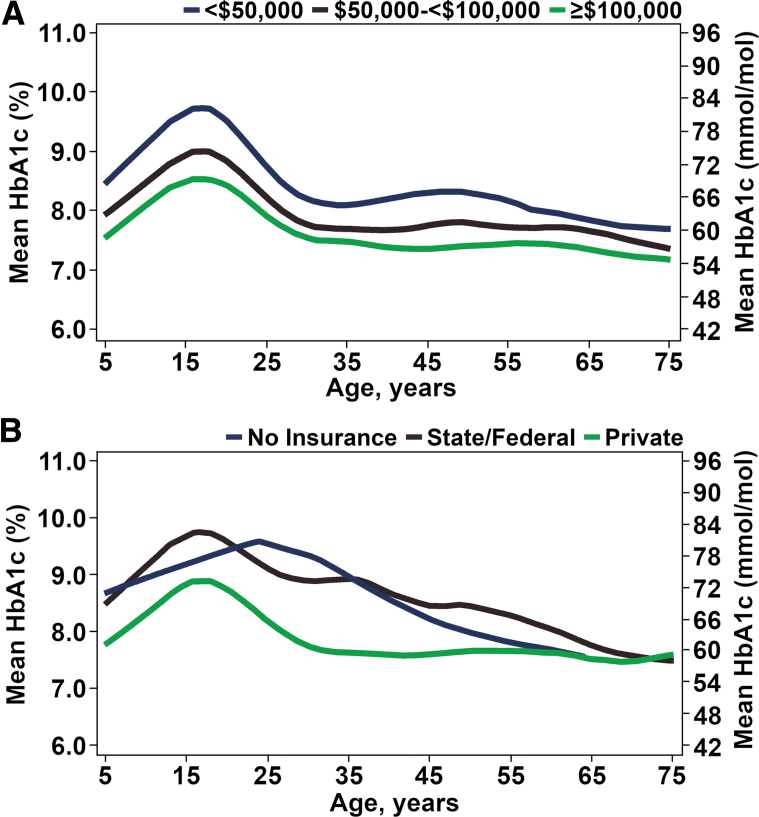
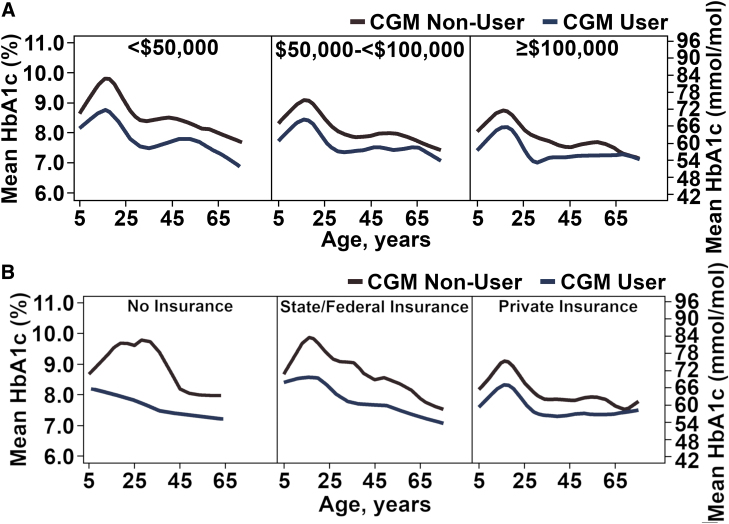
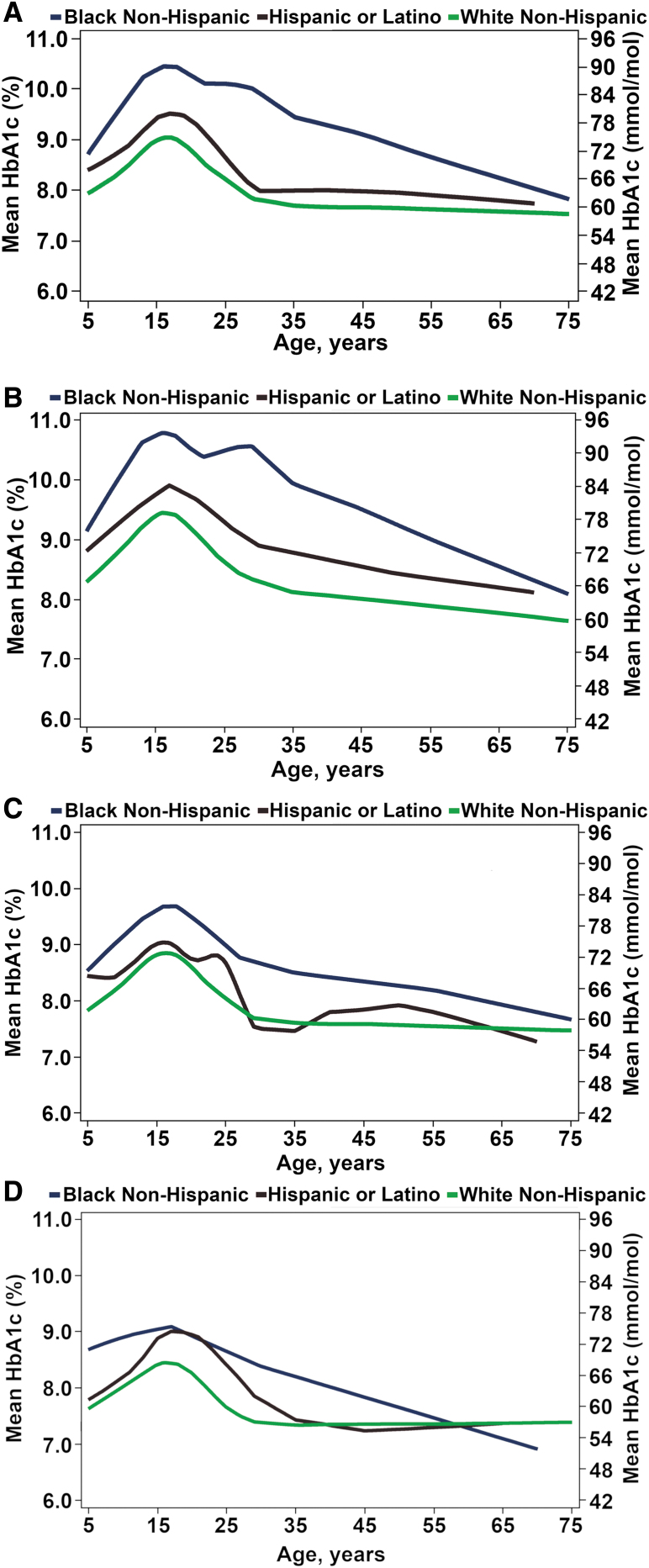
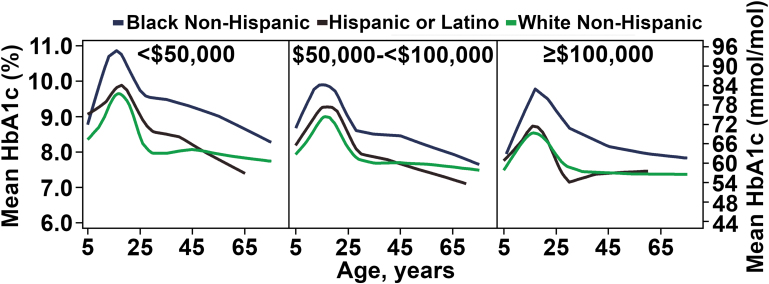
Objective: The T1D Exchange Clinic Registry figure of HbA1c levels according to age has become a classic picture of how average HbA1c varies from childhood to elderly. To further assess the course of HbA1c across the life span in T1D, we created similar figures stratified by device use and socioeconomic status (SES). Methods: Mean HbA1c was plotted versus age for 21,253 T1D Exchange Clinic Registry participants with an HbA1c measurement between January 1, 2016 and March 31, 2018 according to device use, race/ethnicity, and measures of SES. Results: Across the age range from childhood to elderly, continuous glucose monitoring (CGM) use without an insulin pump had better average HbA1c than pump without CGM; and among CGM users, pump and injection users had similar HbA1c levels. Any device use (pump or CGM) was associated with better HbA1c levels than no device use across the age range. Lower SES and African American race were associated with higher HbA1c across the age range. Across all device use, SES, and race/ethnicity factors, average HbA1c levels were highest in adolescents and young adults. Conclusion: Although the plot of average HbA1c from early childhood to elderly shifts according to device use and SES factors, the shape of the plots remains reasonably constant with highest HbA1c levels in adolescents and young adults. These findings emphasize the importance of targeting adolescence and early adulthood as the ages with the greatest need for improving diabetes management irrespective of device use and SES.
Keywords: HbA1c; T1D Exchange; Type 1 diabetes.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Beck RW, Tamborlane WV, Bergenstal RM, et al. : The T1D exchange clinic registry. J Clin Endocrinol Metab 2012;97:4383–4389 - PubMed
-
- Miller KM, Foster NC, Beck RW, et al. : Current state of type 1 diabetes treatment in the U.S.: updated data from the T1D exchange clinic registry. Diabetes Care 2015;38:971–978 - PubMed
-
- Blackman SM, Raghinaru D, Adi S, et al. : Insulin pump use in young children in the T1D exchange clinic registry is associated with lower hemoglobin A1c levels than injection therapy. Pediatr Diabetes 2014;15:564–572 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
