

Pharmacist-Physician Collaboration to Improve the Accuracy of Medication Information in Electronic Medical Discharge Summaries: Effectiveness and Sustainability
- PMID: 31905902
- PMCID: PMC7151653
- DOI: 10.3390/pharmacy8010002
Pharmacist-Physician Collaboration to Improve the Accuracy of Medication Information in Electronic Medical Discharge Summaries: Effectiveness and Sustainability
Abstract
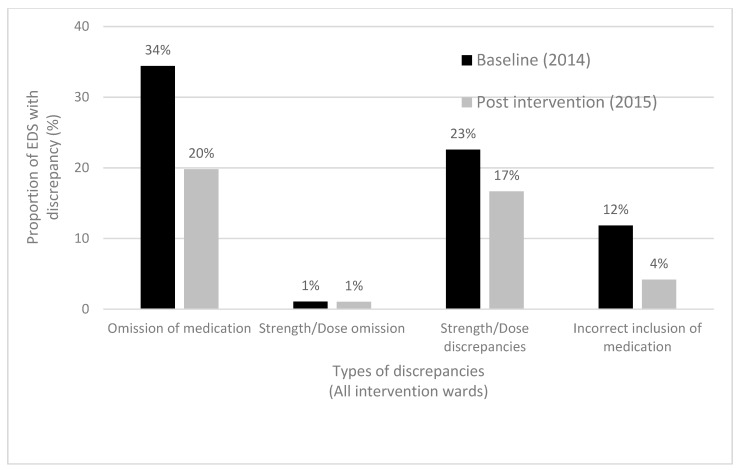
Inaccurate or missing medication information in medical discharge summaries is a widespread and intractable problem. This study evaluated the effectiveness and sustainability of an intervention in which ward-based hospital pharmacists reviewed, contributed and verified medication information in electronic discharge summaries (EDSs) in collaboration with physicians. Retrospective audits of randomly selected EDSs were conducted on seven wards at a major public hospital before and after implementation of the intervention and repeated two years later on four wards where the intervention was incorporated into usual pharmacist care. EDSs for 265 patients (prescribed a median of nine discharge medications) were assessed across the three time points. Pharmacists verified the EDSs for 47% patients in the first post-intervention audit and 68% patients in the second post-intervention audit. Following the intervention, the proportion of patients with one or more clinically significant discharge medication list discrepancy fell from 40/93 (43%) to 14/92 (15%), p < 0.001. The proportion of clinically significant medication changes stated in the EDSs increased from 222/417 (53%) to 296/366 (81%), p < 0.001, and the proportion both stated and explained increased from 206/417 (49%) to 245/366 (67%), p < 0.001. Significant improvements were still evident after two years. Pharmacists spent a median of 5 (range 2-16) minutes per patient contributing to EDSs. Logistics, timing and pharmacist workload were barriers to delivering the intervention. Additional staff resources is needed to enable pharmacists to consistently deliver this effective intervention.
Keywords: care transition; patient discharge summaries; patient transfer; pharmacists.
Conflict of interest statement
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
An audit of the accuracy of medication information in electronic medical discharge summaries linked to an electronic prescribing system.Health Inf Manag. 2018 Sep;47(3):125-131. doi: 10.1177/1833358318765192. Epub 2018 Mar 27. Health Inf Manag. 2018. PMID: 29587532
-
Improving communication of medication changes using a pharmacist-prepared discharge medication management summary.Int J Clin Pharm. 2017 Apr;39(2):394-402. doi: 10.1007/s11096-017-0435-5. Epub 2017 Mar 11. Int J Clin Pharm. 2017. PMID: 28285390
-
Slick scripts: impact on patient flow targets of pharmacists preparing discharge prescriptions in a hospital with an electronic prescribing system.J Eval Clin Pract. 2017 Apr;23(2):333-339. doi: 10.1111/jep.12615. Epub 2016 Aug 15. J Eval Clin Pract. 2017. PMID: 27524695
-
Accuracy of pharmacist electronic discharge medicines review information transmitted to primary care at discharge.Int J Clin Pharm. 2019 Jun;41(3):820-824. doi: 10.1007/s11096-019-00835-1. Epub 2019 Apr 26. Int J Clin Pharm. 2019. PMID: 31028594
-
A Medical Resident-Pharmacist Collaboration Improves the Rate of Medication Reconciliation Verification at Discharge.Jt Comm J Qual Patient Saf. 2015 Oct;41(10):457-61. doi: 10.1016/s1553-7250(15)41059-1. Jt Comm J Qual Patient Saf. 2015. PMID: 26404074
Cited by
-
Personal Electronic Records of Medications (PERMs) for medication reconciliation at care transitions: a rapid realist review.BMC Med Inform Decis Mak. 2021 Nov 3;21(1):307. doi: 10.1186/s12911-021-01659-8. BMC Med Inform Decis Mak. 2021. PMID: 34732176 Free PMC article. Review.
-
Achieving safe medication management during transitions of care from hospital: time for a stewardship approach.Aust Prescr. 2024 Aug;47(4):106-108. doi: 10.18773/austprescr.2024.034. Aust Prescr. 2024. PMID: 39228459 Free PMC article. No abstract available.
-
The complexities of communication at hospital discharge of older patients: a qualitative study of healthcare professionals' views.BMC Health Serv Res. 2023 Nov 6;23(1):1211. doi: 10.1186/s12913-023-10192-5. BMC Health Serv Res. 2023. PMID: 37932683 Free PMC article.
-
Improved Medication communication and Patient involvement At Care Transitions (IMPACT-care): study protocol for a pre-post intervention trial in older hospitalised patients.BMJ Open. 2025 May 2;15(5):e099547. doi: 10.1136/bmjopen-2025-099547. BMJ Open. 2025. PMID: 40316362 Free PMC article.
-
Identifying Medication Review Topics to Be Documented in a Structured Form in Electronic Health Record Systems: Delphi Consensus Survey.J Med Internet Res. 2025 May 6;27:e70133. doi: 10.2196/70133. J Med Internet Res. 2025. PMID: 40328443 Free PMC article.
References
-
- Australian Commission on Safety and Quality in Health Care and NSW Therapeutic Advisory Group Inc. National Quality Use of Medicines Indicators for Australian Hospitals. ACSQHC; Sydney, Australia: 2014. [(accessed on 27 December 2019)]. Available online: https://www.safetyandquality.gov.au/our-work/medication-safety/national-....
-
- Kripalani S., LeFevre F., Phillips C.O., Williams M.V., Basaviah P., Baker D.W. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. JAMA. 2007;297:831–841. doi: 10.1001/jama.297.8.831. - DOI - PubMed
LinkOut - more resources
Full Text Sources
