

Differences in Simulated Refractive Outcomes of Photorefractive Keratectomy (PRK) and Laser In-Situ Keratomileusis (LASIK) for Myopia in Same-Eye Virtual Trials
- PMID: 31906169
- PMCID: PMC6982132
- DOI: 10.3390/ijerph17010287
Differences in Simulated Refractive Outcomes of Photorefractive Keratectomy (PRK) and Laser In-Situ Keratomileusis (LASIK) for Myopia in Same-Eye Virtual Trials
Abstract
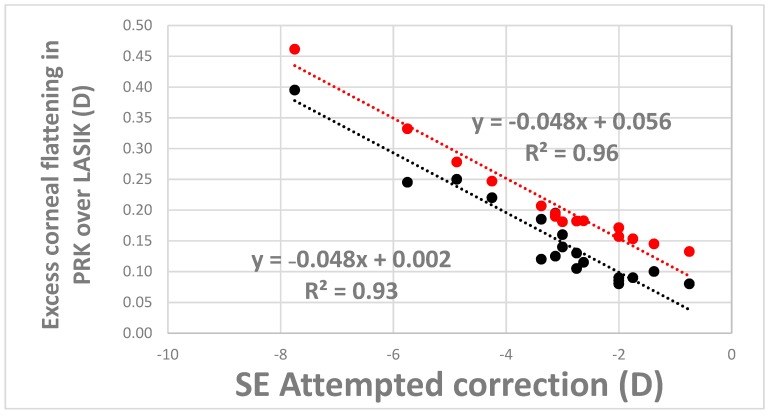
The use of computational mechanics for assessing the structural and optical consequences of corneal refractive procedures is increasing. In practice, surgeons who elect to perform PRK rather than LASIK must often reduce the programmed refractive treatment magnitude to avoid overcorrection of myopia. Building on a recent clinical validation study of finite element analysis (FEA)-based predictions of LASIK outcomes, this study compares predicted responses in the validated LASIK cases to theoretical PRK treatments for the same refractive error. Simulations in 20 eyes demonstrated that PRK resulted in a mean overcorrection of 0.17 ± 0.10 D relative to LASIK and that the magnitude of overcorrection increased as a function of attempted correction. This difference in correction closely matched (within 0.06 ± 0.03 D) observed differences in PRK and LASIK from a historical nomogram incorporating thousands of cases. The surgically induced corneal strain was higher in LASIK than PRK and resulted in more forward displacement of the central stroma and, consequently, less relative flattening in LASIK. This FE model provides structural confirmation of a mechanism of action for the difference in refractive outcomes of these two keratorefractive techniques, and the results were in agreement with empirical clinical data.
Keywords: cornea; finite element analysis; laser in situ keratomileusis (LASIK); photorefractive keratectomy (PRK); refractive surgery.
Conflict of interest statement
W.J.D.: Cleveland Clinic/OptoQuest (Intellectual property), Alcon (clinical research funding); J.S.L.: OptoQuest (employee); I.S.: OptoQuest (consultant).
Figures





References
-
- Maurice D. The Cornea and the Sclera. Academic Press; Cambridge, MA, USA: 1985.
-
- Roberts C. The cornea is not a piece of plastic. J. Refract. Surg. 2001;16:407–413. - PubMed
-
- Dupps W.J., Jr., Roberts C. Effect of acute biomechanical changes on corneal curvature after photokeratectomy. J. Refract. Surg. 2001;17:658–669. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources