

Efficacy and safety of gastrointestinal bleeding prophylaxis in critically ill patients: systematic review and network meta-analysis
- PMID: 31907166
- PMCID: PMC7190057
- DOI: 10.1136/bmj.l6744
Efficacy and safety of gastrointestinal bleeding prophylaxis in critically ill patients: systematic review and network meta-analysis
Abstract
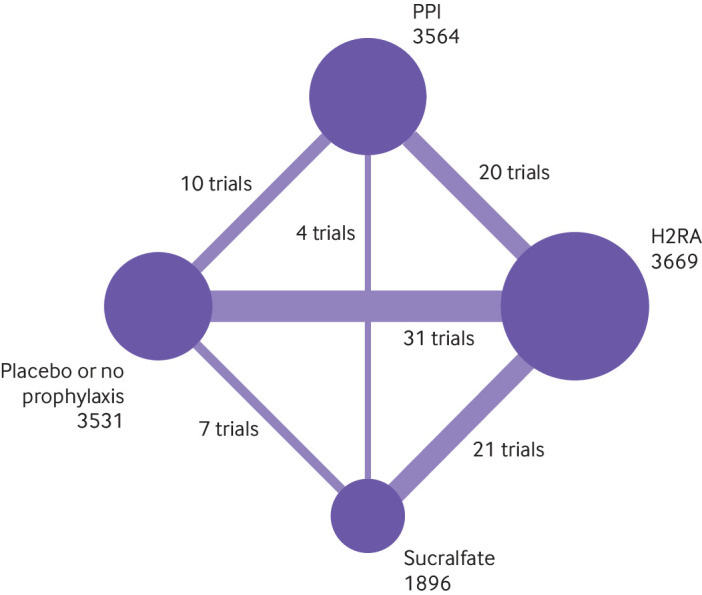
Objective: To determine, in critically ill patients, the relative impact of proton pump inhibitors (PPIs), histamine-2 receptor antagonists (H2RAs), sucralfate, or no gastrointestinal bleeding prophylaxis (or stress ulcer prophylaxis) on outcomes important to patients.
Design: Systematic review and network meta-analysis.
Data sources: Medline, PubMed, Embase, Cochrane Central Register of Controlled Trials, trial registers, and grey literature up to March 2019.
Eligibility criteria for selecting studies and methods: We included randomised controlled trials that compared gastrointestinal bleeding prophylaxis with PPIs, H2RAs, or sucralfate versus one another or placebo or no prophylaxis in adult critically ill patients. Two reviewers independently screened studies for eligibility, extracted data, and assessed risk of bias. A parallel guideline committee (BMJ Rapid Recommendation) provided critical oversight of the systematic review, including identifying outcomes important to patients. We performed random-effects pairwise and network meta-analyses and used GRADE to assess certainty of evidence for each outcome. When results differed between low risk and high risk of bias studies, we used the former as best estimates.
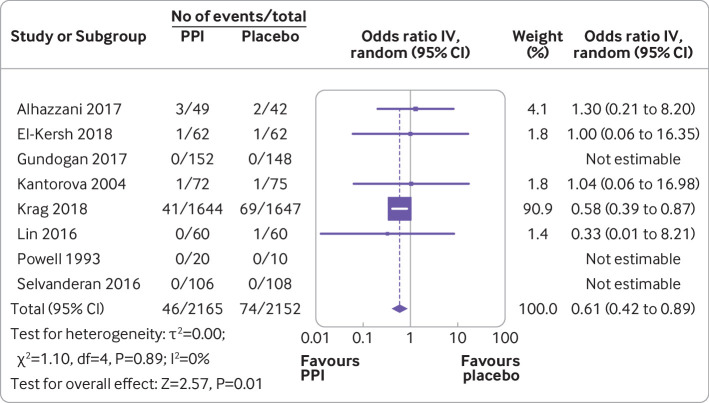
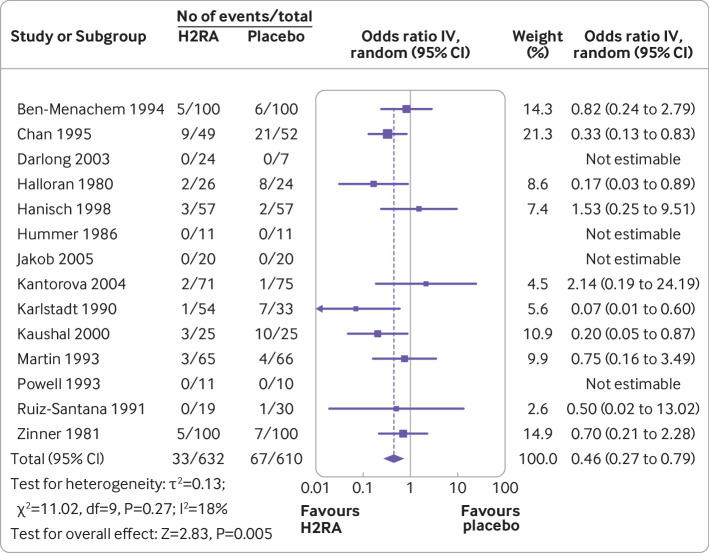
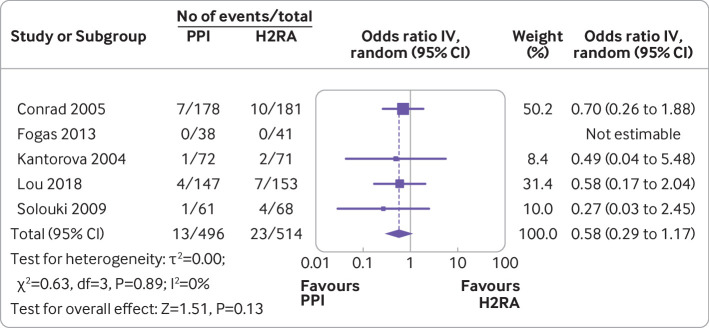
Results: Seventy two trials including 12 660 patients proved eligible. For patients at highest risk (>8%) or high risk (4-8%) of bleeding, both PPIs and H2RAs probably reduce clinically important gastrointestinal bleeding compared with placebo or no prophylaxis (odds ratio for PPIs 0.61 (95% confidence interval 0.42 to 0.89), 3.3% fewer for highest risk and 2.3% fewer for high risk patients, moderate certainty; odds ratio for H2RAs 0.46 (0.27 to 0.79), 4.6% fewer for highest risk and 3.1% fewer for high risk patients, moderate certainty). Both may increase the risk of pneumonia compared with no prophylaxis (odds ratio for PPIs 1.39 (0.98 to 2.10), 5.0% more, low certainty; odds ratio for H2RAs 1.26 (0.89 to 1.85), 3.4% more, low certainty). It is likely that neither affect mortality (PPIs 1.06 (0.90 to 1.28), 1.3% more, moderate certainty; H2RAs 0.96 (0.79 to 1.19), 0.9% fewer, moderate certainty). Otherwise, results provided no support for any affect on mortality, Clostridium difficile infection, length of intensive care stay, length of hospital stay, or duration of mechanical ventilation (varying certainty of evidence).
Conclusions: For higher risk critically ill patients, PPIs and H2RAs likely result in important reductions in gastrointestinal bleeding compared with no prophylaxis; for patients at low risk, the reduction in bleeding may be unimportant. Both PPIs and H2RAs may result in important increases in pneumonia. Variable quality evidence suggested no important effects of interventions on mortality or other in-hospital morbidity outcomes.
Systematic review registration: PROSPERO CRD42019126656.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; AP and MHM are the co-authors of the SUP-ICU trial (doi:10.1056/NEJMoa1714919); GHG is one of the investigators of the REVISE trial. There are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Comment in
-
Gastrointestinal bleeding prophylaxis for critically ill patients: a clinical practice guideline.BMJ. 2020 Jan 6;368:l6722. doi: 10.1136/bmj.l6722. BMJ. 2020. PMID: 31907223
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical