

High-Dose Chloroquine for Uncomplicated Plasmodium falciparum Malaria Is Well Tolerated and Causes Similar QT Interval Prolongation as Standard-Dose Chloroquine in Children
- PMID: 31907183
- PMCID: PMC7038251
- DOI: 10.1128/AAC.01846-19
High-Dose Chloroquine for Uncomplicated Plasmodium falciparum Malaria Is Well Tolerated and Causes Similar QT Interval Prolongation as Standard-Dose Chloroquine in Children
Abstract
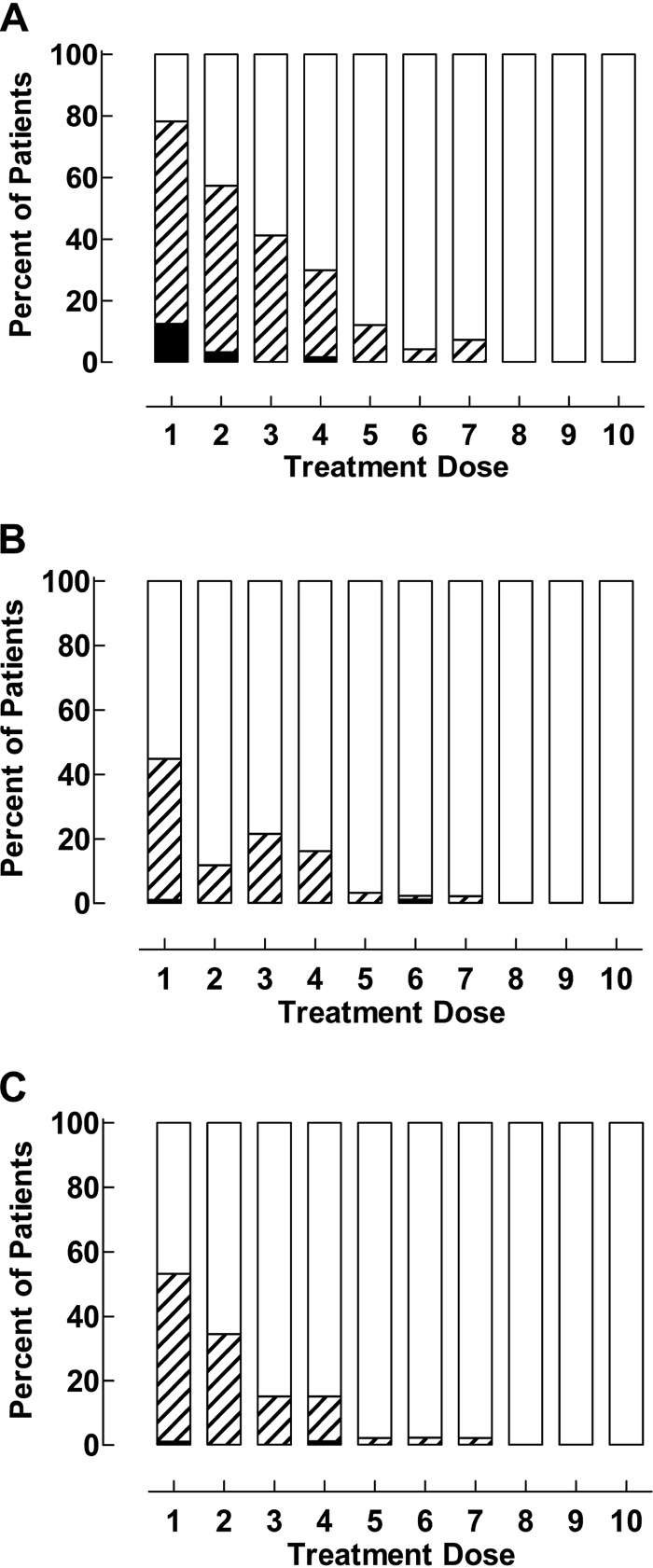
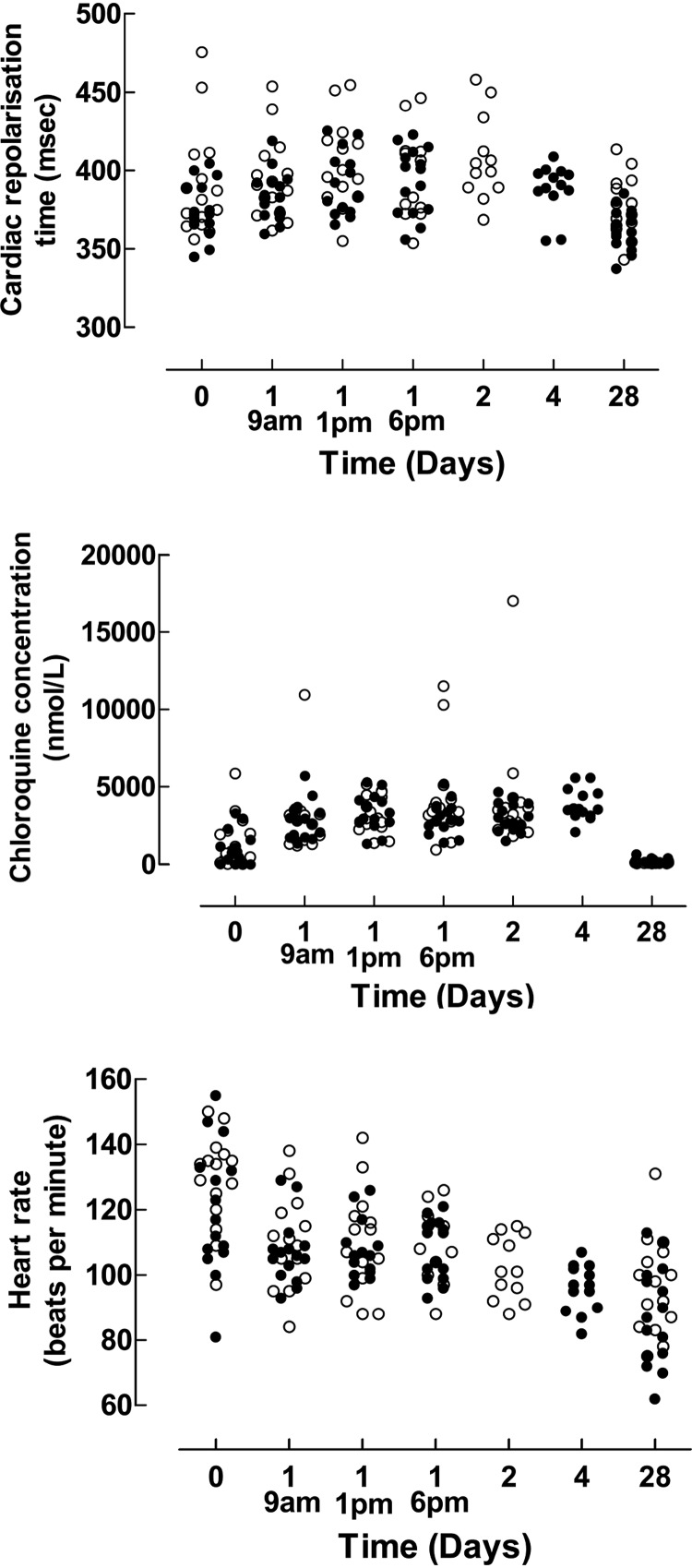
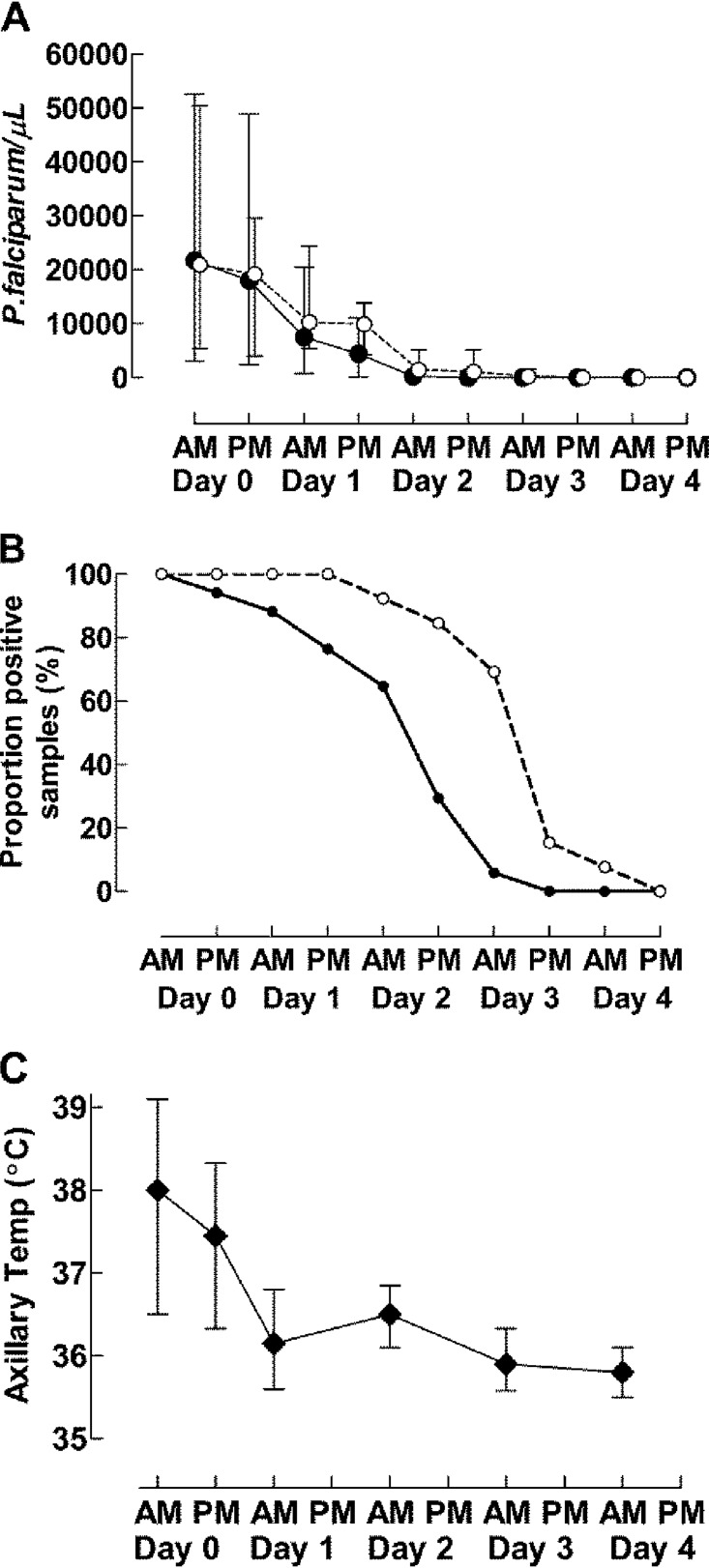
Higher chloroquine doses can effectively treat up to 93 to 96% of malaria infections caused by Plasmodium falciparum carrying the resistance-conferring chloroquine resistance transporter (pfcrt) 76T allele. The tolerability of 50 (double the standard dose) and 70 mg/kg total chloroquine doses were assessed in this study. Fifteen 4- to 8-year-old children with uncomplicated malaria were given 10 mg/kg of chloroquine twice daily for 2 days and 5 mg/kg twice daily on the third day. Fifteen additional children were given 5 mg/kg twice daily for 2 more days. Chloroquine concentrations, blood pressure, electrocardiograms (ECGs), parasite density, and adverse events were assessed until day 28. Both dosages were well tolerated, and symptoms resolved by day 3 in parallel with increasing chloroquine concentrations. The median corrected QT (QTc) interval was 12 to 26 ms higher at expected peak concentrations than at day 0 (P < 0.001). Pfcrt 76T was associated with delayed parasite clearance. Day 28 clinical and parasitological responses against P. falciparum with pfcrt 76T were 57% (4/7) and 67% (4/6) after treatment with 50 and 70 mg/kg, respectively. Dosages were well tolerated, and no severe cardiac adverse events occurred. The QTc interval increase was similar to that found in adults taking 25 mg/kg of chloroquine. (This study has been registered at ClinicalTrials.gov under identifier NCT01814423.).
Keywords: Guinea-Bissau; Plasmodium falciparum; cardiac safety; chloroquine; pfcrt; pharmacokinetics; tolerability; treatment.
Copyright © 2020 American Society for Microbiology.
Figures
References
-
- World Health Organization. 2015. Guidelines for the treatment of malaria, 5th ed World Health Organization, Geneva, Switzerland: http://www.who.int/malaria/publications/atoz/9789241549127/en/.
-
- Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, Lwin KM, Ariey F, Hanpithakpong W, Lee SJ, Ringwald P, Silamut K, Imwong M, Chotivanich K, Lim P, Herdman T, An SS, Yeung S, Singhasivanon P, Day NP, Lindegardh N, Socheat D, White NJ. 2009. Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 361:455–467. doi: 10.1056/NEJMoa0808859. - DOI - PMC - PubMed
-
- Summers RL, Dave A, Dolstra TJ, Bellanca S, Marchetti RV, Nash MN, Richards SN, Goh V, Schenk RL, Stein WD, Kirk K, Sanchez CP, Lanzer M, Martin RE. 2014. Diverse mutational pathways converge on saturable chloroquine transport via the malaria parasite’s chloroquine resistance transporter. Proc Natl Acad Sci U S A 111:E1759-67. doi: 10.1073/pnas.1322965111. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
