

Phantom-based image quality assessment of clinical 18F-FDG protocols in digital PET/CT and comparison to conventional PMT-based PET/CT
- PMID: 31907664
- PMCID: PMC6944719
- DOI: 10.1186/s40658-019-0269-4
Phantom-based image quality assessment of clinical 18F-FDG protocols in digital PET/CT and comparison to conventional PMT-based PET/CT
Abstract
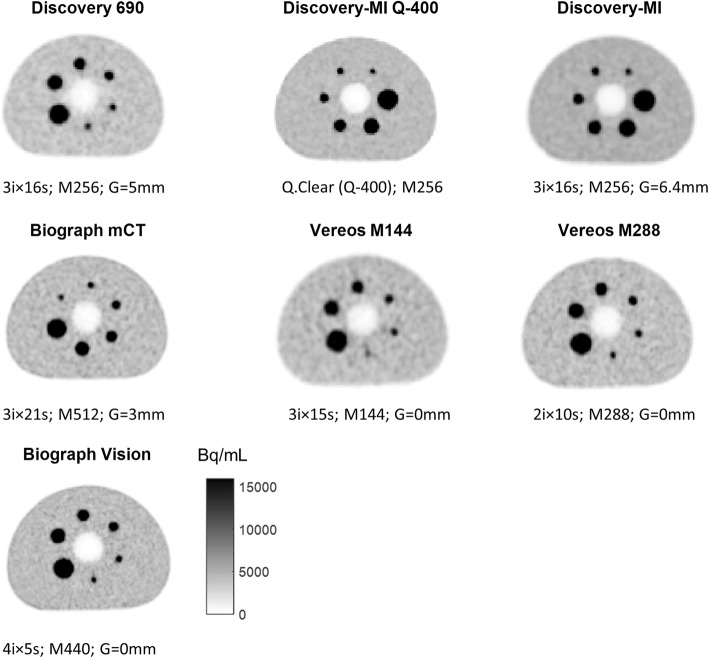
Background: We assessed and compared image quality obtained with clinical 18F-FDG whole-body oncologic PET protocols used in three different, state-of-the-art digital PET/CT and two conventional PMT-based PET/CT devices. Our goal was to evaluate an improved trade-off between administered activity (patient dose exposure/signal-to-noise ratio) and acquisition time (patient comfort) while preserving diagnostic information achievable with the recently introduced digital detector technology compared to previous analogue PET technology.
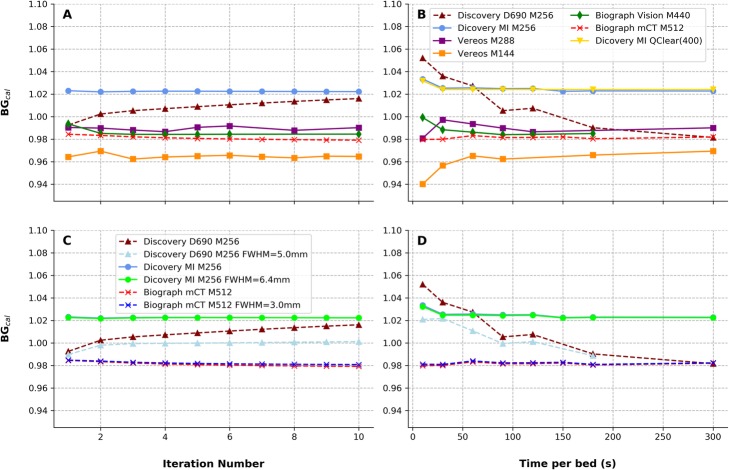
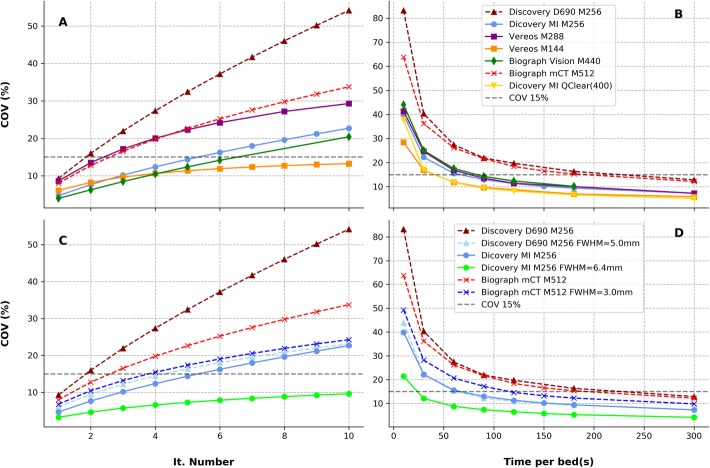
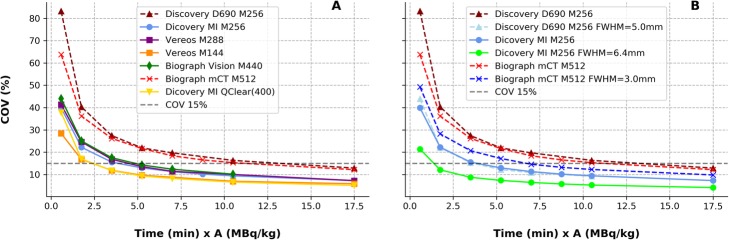
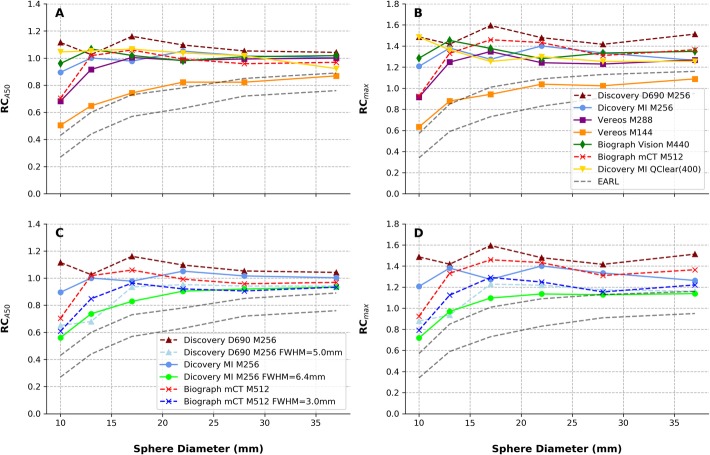
Methods: We performed list-mode (LM) PET acquisitions using a NEMA/IEC NU2 phantom, with activity concentrations of 5 kBq/mL and 25 kBq/mL for the background (9.5 L) and sphere inserts, respectively. For each device, reconstructions were obtained varying the image statistics (10, 30, 60, 90, 120, 180, and 300 s from LM data) and the number of iterations (range 1 to 10) in addition to the employed local clinical protocol setup. We measured for each reconstructed dataset: the quantitative cross-calibration, the image noise on the uniform background assessed by the coefficient of variation (COV), and the recovery coefficients (RCs) evaluated in the hot spheres. Additionally, we compared the characteristic time-activity-product (TAP) that is the product of scan time per bed position × mass-activity administered (in min·MBq/kg) across datasets.
Results: Good system cross-calibration was obtained for all tested datasets with < 6% deviation from the expected value was observed. For all clinical protocol settings, image noise was compatible with clinical interpretation (COV < 15%). Digital PET showed an improved background signal-to-noise ratio as compared to conventional PMT-based PET. RCs were comparable between digital and PMT-based PET datasets. Compared to PMT-based PET, digital systems provided comparable image quality with lower TAP (from ~ 40% less and up to 70% less).
Conclusions: This study compared the achievable clinical image quality in three state-of-the-art digital PET/CT devices (from different vendors) as well as in two conventional PMT-based PET. Reported results show that a comparable image quality is achievable with a TAP reduction of ~ 40% in digital PET. This could lead to a significant reduction of the administered mass-activity and/or scan time with direct benefits in terms of dose exposure and patient comfort.
Keywords: Digital PET/CT; Dose reduction; Image quality; Protocol optimization.
Conflict of interest statement
The authors declare that they have no competing interests
Figures
Similar articles
-
Phantom-based acquisition time and image reconstruction parameter optimisation for oncologic FDG PET/CT examinations using a digital system.BMC Cancer. 2022 Aug 18;22(1):899. doi: 10.1186/s12885-022-09993-4. BMC Cancer. 2022. PMID: 35978274 Free PMC article.
-
Total-body 18F-FDG PET/CT scan in oncology patients: how fast could it be?Eur J Nucl Med Mol Imaging. 2021 Jul;48(8):2384-2394. doi: 10.1007/s00259-021-05357-5. Epub 2021 Apr 18. Eur J Nucl Med Mol Imaging. 2021. PMID: 33866409
-
Image Quality and Activity Optimization in Oncologic 18F-FDG PET Using the Digital Biograph Vision PET/CT System.J Nucl Med. 2020 May;61(5):764-771. doi: 10.2967/jnumed.119.234351. Epub 2019 Oct 18. J Nucl Med. 2020. PMID: 31628214
-
Performance Evaluation of the Vereos PET/CT System According to the NEMA NU2-2012 Standard.J Nucl Med. 2019 Apr;60(4):561-567. doi: 10.2967/jnumed.118.215541. Epub 2018 Oct 25. J Nucl Med. 2019. PMID: 30361382
-
Optimal clinical protocols for total-body 18F-FDG PET/CT examination under different activity administration plans.EJNMMI Phys. 2023 Feb 18;10(1):14. doi: 10.1186/s40658-023-00533-y. EJNMMI Phys. 2023. PMID: 36808378 Free PMC article.
Cited by
-
Simultaneous evaluation of brain metastasis and thoracic cancer using semiconductor 11C-methionine PET/CT imaging.Ann Nucl Med. 2024 Apr;38(4):278-287. doi: 10.1007/s12149-024-01908-6. Epub 2024 Feb 22. Ann Nucl Med. 2024. PMID: 38386272
-
Fully digital PET is unaffected by any deterioration in TOF resolution and TOF image quality in the wide range of routine PET count rates.EJNMMI Phys. 2021 Jan 6;8(1):1. doi: 10.1186/s40658-020-00344-5. EJNMMI Phys. 2021. PMID: 33409746 Free PMC article.
-
BSREM for Brain Metastasis Detection with 18F-FDG-PET/CT in Lung Cancer Patients.J Digit Imaging. 2022 Jun;35(3):581-593. doi: 10.1007/s10278-021-00570-y. Epub 2022 Feb 25. J Digit Imaging. 2022. PMID: 35212859 Free PMC article.
-
Shining Damaged Hearts: Immunotherapy-Related Cardiotoxicity in the Spotlight of Nuclear Cardiology.Int J Mol Sci. 2022 Mar 30;23(7):3802. doi: 10.3390/ijms23073802. Int J Mol Sci. 2022. PMID: 35409161 Free PMC article. Review.
-
Phantom-based acquisition time and image reconstruction parameter optimisation for oncologic FDG PET/CT examinations using a digital system.BMC Cancer. 2022 Aug 18;22(1):899. doi: 10.1186/s12885-022-09993-4. BMC Cancer. 2022. PMID: 35978274 Free PMC article.
References
-
- Herholz K. The role of PET quantification in neurological imaging: FDG and amyloid imaging in dementia. Clin Transl Imaging. 2014;2(4):321–330. doi: 10.1007/s40336-014-0073-z. - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
