

The Association of Public Insurance with Postpartum Contraception Preference and Provision
- PMID: 31908549
- PMCID: PMC6927572
- DOI: 10.2147/OAJC.S231196
The Association of Public Insurance with Postpartum Contraception Preference and Provision
Abstract
Background: Prior studies have noted that public insurance status is associated with increased uptake of postpartum contraception whereas others have pointed to public insurance as a barrier to accessing highly effective forms of contraception.
Objective: To assess differences in planned method and provision of postpartum contraception according to insurance type.
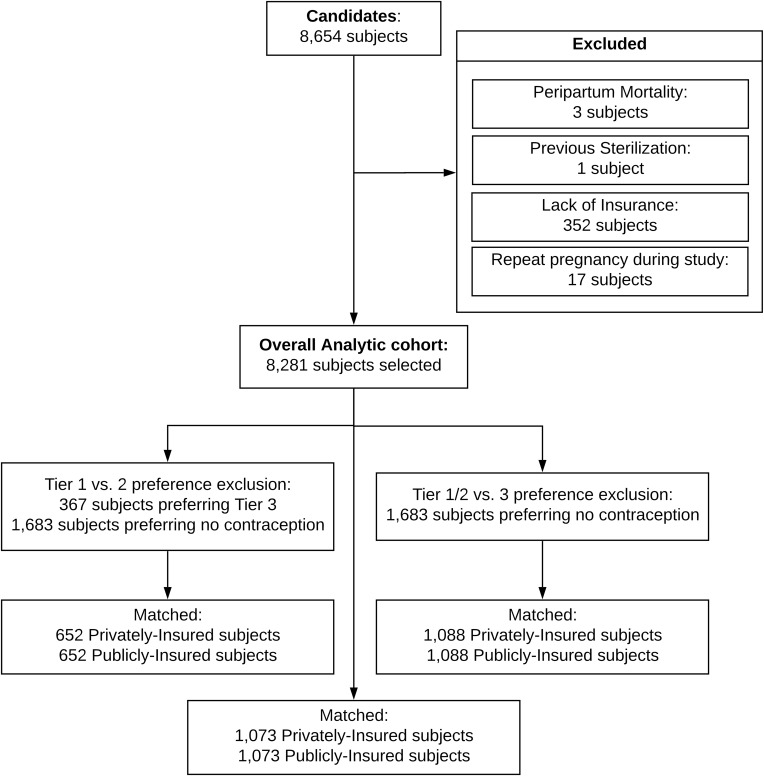
Study design: This is a secondary analysis of a retrospective cohort study examining postpartum women delivered at a single hospital in Cleveland, Ohio from 2012-2014. Contraceptive methods were analyzed according to Tier-based effectiveness as defined by the Centers for Disease Control and Prevention. The primary outcome was postpartum contraception method preference. Additional outcomes included method provision, postpartum visit attendance, and subsequent pregnancy within 365 days of delivery.
Results: Of the 8281 patients in the study cohort, 1372 (16.6%) were privately and 6990 (83.4%) were publicly insured. After adjusting for the potentially confounding clinical and demographic factors through propensity score analysis, public insurance was not associated with preference for a Tier 1 versus Tier 2 postpartum contraceptive method (matched adjusted odds ratio [maOR] 0.89, 95% CI 0.69-1.15), but was associated with a preference for Tier 1/2 vs Tier 3/None (maOR 1.41, 95% CI 1.17-1.69). There was no difference between women with private or public insurance in terms of method provision by 90 days after delivery (maOR 0.94, 95% CI 0.75-1.17). Public insurance status was also associated with decreased postpartum visit attendance (maOR 0.54, 95% CI 0.43-0.68) and increased rates of subsequent pregnancy within 365 days of delivery (maOR 1.29, 95% CI 1.05-1.59).
Conclusion: Public insurance status does not serve as a barrier to either the preference or provision of effective postpartum contraception. Women desiring highly- or moderately effective methods of contraception should have these methods provided prior to hospital discharge to minimize barriers to method provision.
Keywords: LARC; Medicaid; disparities; insurance; postpartum contraception; sterilization.
© 2019 Verbus et al.
Conflict of interest statement
Dr. Arora is funded by the Clinical and Translational Science Collaborative of Cleveland, KL2TR0002547 from the National Center for Advancing Translational Sciences (NCATS) component of the National Institutes of Health and NIH roadmap for Medical Research. This manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The authors report no other conflicts of interest.
Figures
Similar articles
-
The impact of the COVID-19 pandemic on postpartum contraception planning.Am J Obstet Gynecol MFM. 2021 Sep;3(5):100412. doi: 10.1016/j.ajogmf.2021.100412. Epub 2021 May 28. Am J Obstet Gynecol MFM. 2021. PMID: 34058421 Free PMC article.
-
Medicaid and receipt of interval postpartum long-acting reversible contraception.Contraception. 2019 Jan;99(1):32-35. doi: 10.1016/j.contraception.2018.08.017. Epub 2018 Sep 5. Contraception. 2019. PMID: 30194927 Free PMC article.
-
Contraception After Delivery Among Publicly Insured Women in Texas: Use Compared With Preference.Obstet Gynecol. 2017 Aug;130(2):393-402. doi: 10.1097/AOG.0000000000002136. Obstet Gynecol. 2017. PMID: 28697112 Free PMC article.
-
Disparities in Postpartum Contraceptive Counseling and Provision Among Mothers of Preterm Infants.J Womens Health (Larchmt). 2018 May;27(5):676-683. doi: 10.1089/jwh.2017.6561. Epub 2018 Jan 23. J Womens Health (Larchmt). 2018. PMID: 29359987 Free PMC article.
-
Desired Sterilization Procedure at the Time of Cesarean Delivery According to Insurance Status.Obstet Gynecol. 2019 Dec;134(6):1171-1177. doi: 10.1097/AOG.0000000000003552. Obstet Gynecol. 2019. PMID: 31764726 Free PMC article.
Cited by
-
Does socioeconomic factors and healthcare coverage affect postpartum sterilization uptake in an urban, tertiary hospital?Reprod Health. 2023 Jan 27;20(1):23. doi: 10.1186/s12978-023-01572-5. Reprod Health. 2023. PMID: 36707807 Free PMC article.
-
Changes in Rates of Inpatient Postpartum Long-Acting Reversible Contraception and Sterilization in the USA, 2012-2016.Matern Child Health J. 2021 Oct;25(10):1562-1573. doi: 10.1007/s10995-021-03152-0. Epub 2021 May 10. Matern Child Health J. 2021. PMID: 33970416 Free PMC article.
-
Shared Decision-Making: The Way Forward for Postpartum Contraceptive Counseling.Open Access J Contracept. 2022 Aug 25;13:121-129. doi: 10.2147/OAJC.S360833. eCollection 2022. Open Access J Contracept. 2022. PMID: 36046227 Free PMC article. Review.
References
-
- Jansa V, Blickstein I, Lucovnik M, Fabjan-Vodusek V, Verdenik I, Tul N. The impact of inter-pregnancy interval on subsequent risk of preterm birth. J Matern-Fetal Neo Med. 2017;11:1–7. - PubMed
-
- World Health Organization. WHO recommendations on postnatal care of the mother and newborn. Geneva, Switzerland: World Health Organization; 2013. - PubMed
-
- Optimizing postpartum care. ACOG committee opinion No. 736. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2019;131:e140–50.
LinkOut - more resources
Full Text Sources
