

Myocardial infarction with non-obstructive coronary arteries: A comprehensive review and future research directions
- PMID: 31908730
- PMCID: PMC6937414
- DOI: 10.4330/wjc.v11.i12.305
Myocardial infarction with non-obstructive coronary arteries: A comprehensive review and future research directions
Abstract
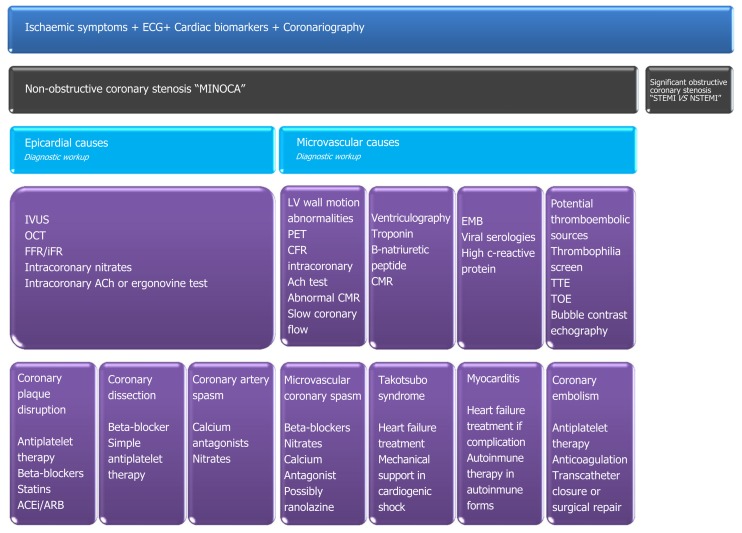
Acute coronary syndromes constitute a variety of myocardial injury presentations that include a subset of patients presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA). This acute coronary syndrome differs from type 1 myocardial infarction (MI) regarding patient characteristics, presentation, physiopathology, management, treatment, and prognosis. Two-thirds of MINOCA subjects present ST-segment elevation; MINOCA patients are younger, are more often female and tend to have fewer cardiovascular risk factors. Moreover, MINOCA is a working diagnosis, and defining the aetiologic mechanism is relevant because it affects patient care and prognosis. In the absence of relevant coronary artery disease, myocardial ischaemia might be triggered by an acute event in epicardial coronary arteries, coronary microcirculation, or both. Epicardial causes of MINOCA include coronary plaque disruption, coronary dissection, and coronary spasm. Microvascular MINOCA mechanisms involve microvascular coronary spasm, takotsubo syndrome (TTS), myocarditis, and coronary thromboembolism. Coronary angiography with non-significant coronary stenosis and left ventriculography are first-line tests in the differential study of MINOCA patients. The diagnostic arsenal includes invasive and non-invasive techniques. Medical history and echocardiography can help indicate vasospasm or thrombosis, if one finite coronary territory is affected, or specify TTS if apical ballooning is present. Intravascular ultrasound, optical coherence tomography, and provocative testing are encouraged. Cardiac magnetic resonance is a cornerstone in myocarditis diagnosis. MINOCA is not a benign diagnosis, and its polymorphic forms differ in prognosis. MINOCA care varies across centres, and future multi-centre clinical trials with standardized criteria may have a positive impact on defining optimal cardiovascular care for MINOCA patients.
Keywords: Management; Myocardial infarction; Myocardial infarction with non-obstructive coronary arteries; Non-obstructive coronary; Prognosis.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest.
Figures
Similar articles
-
Myocardial infarction with non-obstructive coronary arteries (MINOCA): Intracoronary imaging-based diagnosis and management.J Cardiol. 2021 May;77(5):444-451. doi: 10.1016/j.jjcc.2021.01.001. Epub 2021 Jan 16. J Cardiol. 2021. PMID: 33468365 Review.
-
Myocardial infarction with non-obstructive coronary arteries (MINOCA).Front Cardiovasc Med. 2022 Nov 15;9:1032436. doi: 10.3389/fcvm.2022.1032436. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36457805 Free PMC article.
-
Editor's Choice- Pathophysiology, diagnosis and management of MINOCA: an update.Eur Heart J Acute Cardiovasc Care. 2019 Feb;8(1):54-62. doi: 10.1177/2048872618782414. Epub 2018 Jun 28. Eur Heart J Acute Cardiovasc Care. 2019. PMID: 29952633 Review.
-
Case report: assessment and management of myocardial infarction and non-obstructive coronary arteries (MINOCA): the role of microvascular coronary vasospasm.Cardiovasc Diagn Ther. 2019 Aug;9(4):400-405. doi: 10.21037/cdt.2019.07.13. Cardiovasc Diagn Ther. 2019. PMID: 31555546 Free PMC article.
-
[MINOCA-myocardial infarction with non-obstructive coronary arteries].Herz. 2018 Dec;43(8):759-770. doi: 10.1007/s00059-018-4756-5. Herz. 2018. PMID: 30328479 German.
Cited by
-
High versus Low Mechanical Index Imaging Diagnostic Ultrasound in Patients with Myocardial Infarction: A Therapeutic Application Study.Med Sci Monit. 2020 Aug 13;26:e923583. doi: 10.12659/MSM.923583. Med Sci Monit. 2020. PMID: 32790651 Free PMC article.
-
Non-ST-segment elevation myocardial infarction with non-obstructive coronary arteries due to a type-A thymoma: A case report.Heliyon. 2023 Jun 15;9(6):e17317. doi: 10.1016/j.heliyon.2023.e17317. eCollection 2023 Jun. Heliyon. 2023. PMID: 37383184 Free PMC article.
-
Cardiac Magnetic Resonance Imaging as a Risk Stratification Tool in COVID-19 Myocarditis.Diagnostics (Basel). 2024 Apr 10;14(8):790. doi: 10.3390/diagnostics14080790. Diagnostics (Basel). 2024. PMID: 38667436 Free PMC article.
-
Cellular Mechanisms of Coronary Artery Spasm.Biomedicines. 2022 Sep 21;10(10):2349. doi: 10.3390/biomedicines10102349. Biomedicines. 2022. PMID: 36289612 Free PMC article. Review.
-
Association Between Obstructive Sleep Apnea-Hypopnea Syndrome and Outcomes in Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease.Front Cardiovasc Med. 2020 Oct 23;7:573819. doi: 10.3389/fcvm.2020.573819. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 33195461 Free PMC article.
References
-
- Gross H, Sternberg WH. Myocardial infarction without significant lesions of coronary arteries. Arch Intern Med (Chic) 1939;64:249–267.
-
- Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36:959–969. - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018) J Am Coll Cardiol. 2018;72:2231–2264. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimský P ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S ESC Scientific Document Group. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:267–315. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
