

Senescence marker activin A is increased in human diabetic kidney disease: association with kidney function and potential implications for therapy
- PMID: 31908790
- PMCID: PMC6936543
- DOI: 10.1136/bmjdrc-2019-000720
Senescence marker activin A is increased in human diabetic kidney disease: association with kidney function and potential implications for therapy
Abstract
Objective: Activin A, an inflammatory mediator implicated in cellular senescence-induced adipose tissue dysfunction and profibrotic kidney injury, may become a new target for the treatment of diabetic kidney disease (DKD) and chronic kidney diseases. We tested the hypothesis that human DKD-related injury leads to upregulation of activin A in blood and urine and in a human kidney cell model. We further hypothesized that circulating activin A parallels kidney injury markers in DKD.
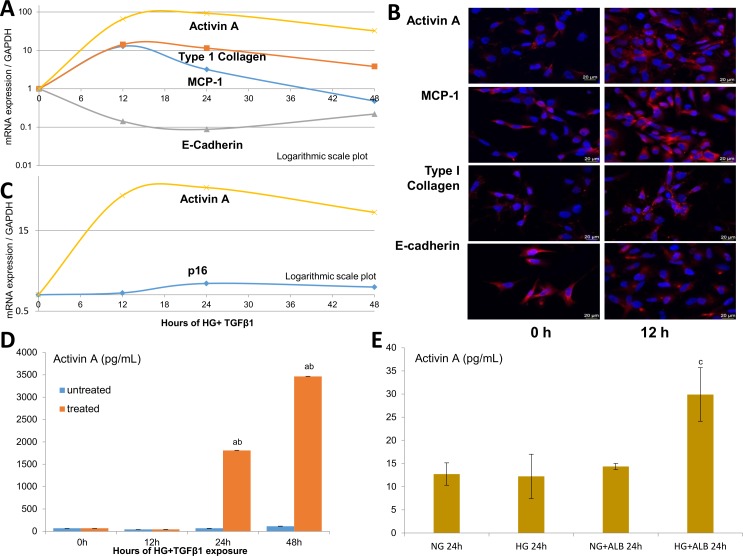
Research design and methods: In two adult diabetes cohorts and controls (Minnesota, USA; Galway, Ireland), the relationships between plasma (or urine) activin A, estimated glomerular filtration rate (eGFR) and DKD injury biomarkers were tested with logistic regression and correlation coefficients. Activin A, inflammatory, epithelial-mesenchymal-transition (EMT) and senescence markers were assayed in human kidney (HK-2) cells incubated in high glucose plus transforming growth factor-β1 or albumin.
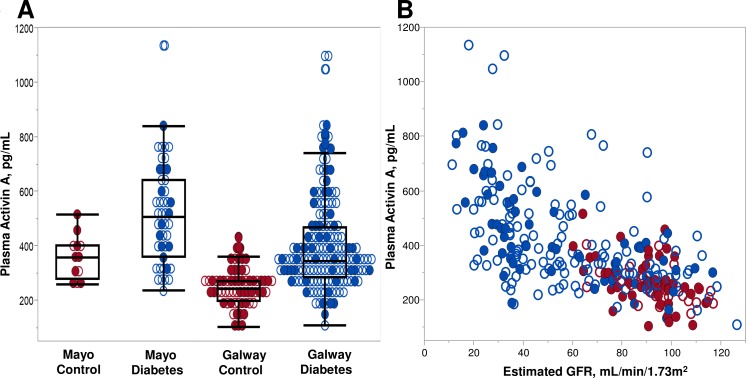
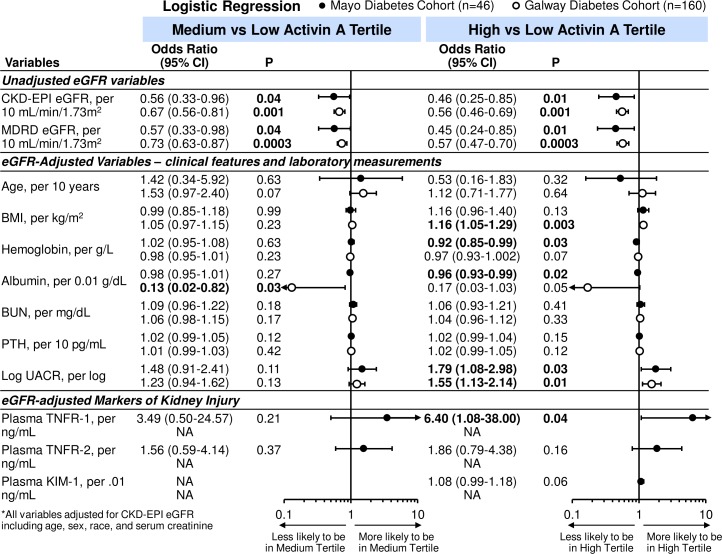
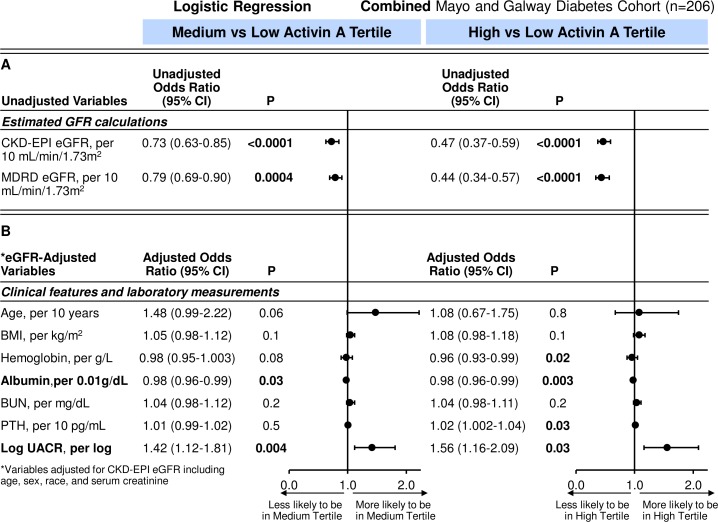
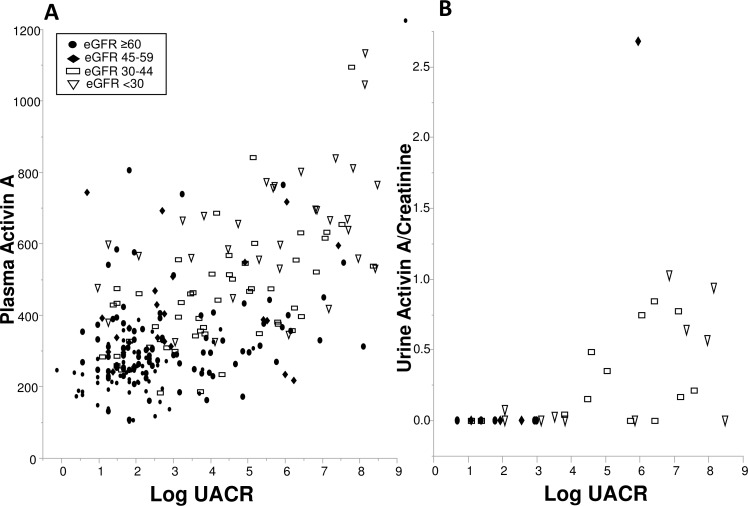
Results: Plasma activin A levels were elevated in diabetes (n=206) compared with controls (n=76; 418.1 vs 259.3 pg/mL; p<0.001) and correlated inversely with eGFR (rs=-0.61; p<0.001; diabetes). After eGFR adjustment, only albuminuria (OR 1.56, 95% CI 1.16 to 2.09) and tumor necrosis factor receptor-1 (OR 6.40, 95% CI 1.08 to 38.00) associated with the highest activin tertile. Albuminuria also related to urinary activin (rs=0.65; p<0.001). Following in vitro HK-2 injury, activin, inflammatory, EMT genes and supernatant activin levels were increased.
Conclusions: Circulating activin A is increased in human DKD and correlates with reduced kidney function and kidney injury markers. DKD-injured human renal tubule cells develop a profibrotic and inflammatory phenotype with activin A upregulation. These findings underscore the role of inflammation and provide a basis for further exploration of activin A as a diagnostic marker and therapeutic target in DKD.
Keywords: adipocytokine; clinical aspects of diabetes; clinical nephrology; renal fibrosis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous