

Prediction on the plantar fascia strain offload upon Fascia taping and Low-Dye taping during running
- PMID: 31908942
- PMCID: PMC6938939
- DOI: 10.1016/j.jot.2019.06.006
Prediction on the plantar fascia strain offload upon Fascia taping and Low-Dye taping during running
Abstract
Background: Taping is commonly prescribed to treat plantar fasciitis for runners by virtue of its alleged ability to offload the plantar fascia and facilitate positive injury prognosis. Our study aimed to investigate how different taping methods could change the loading on the plantar fascia during running using computational simulations.
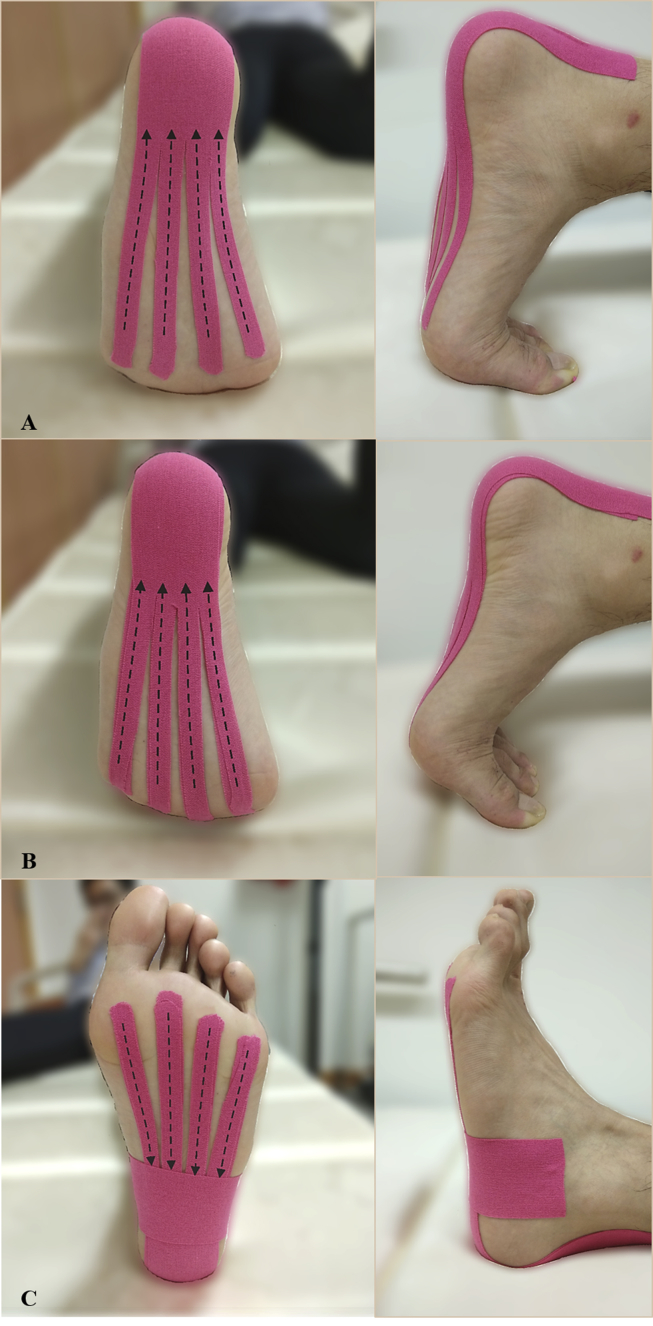
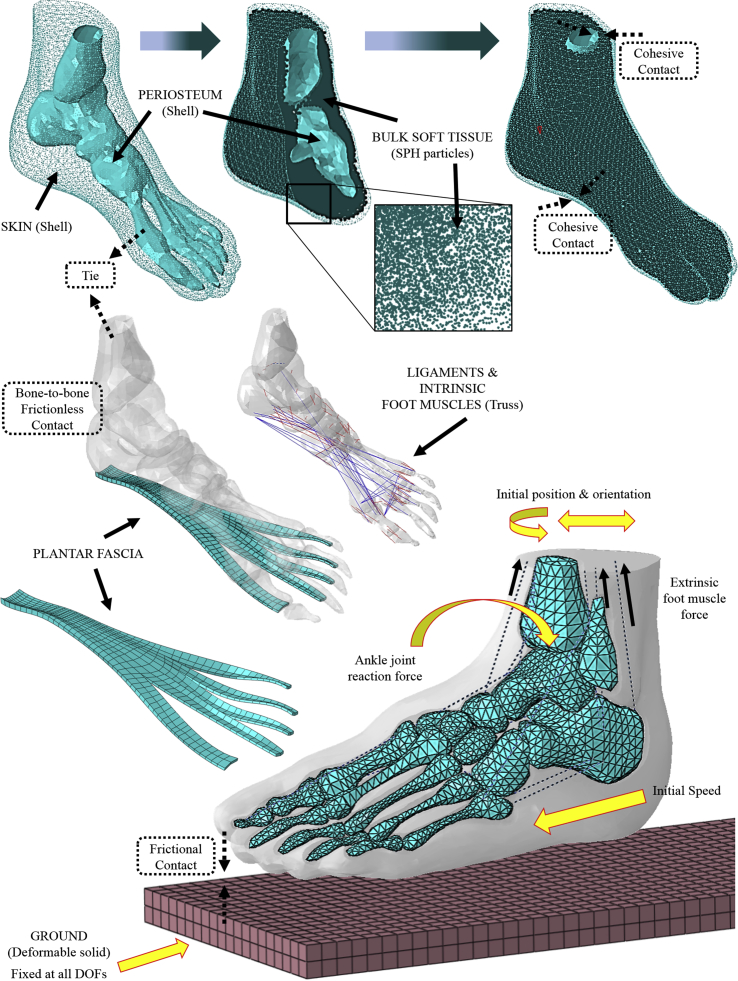
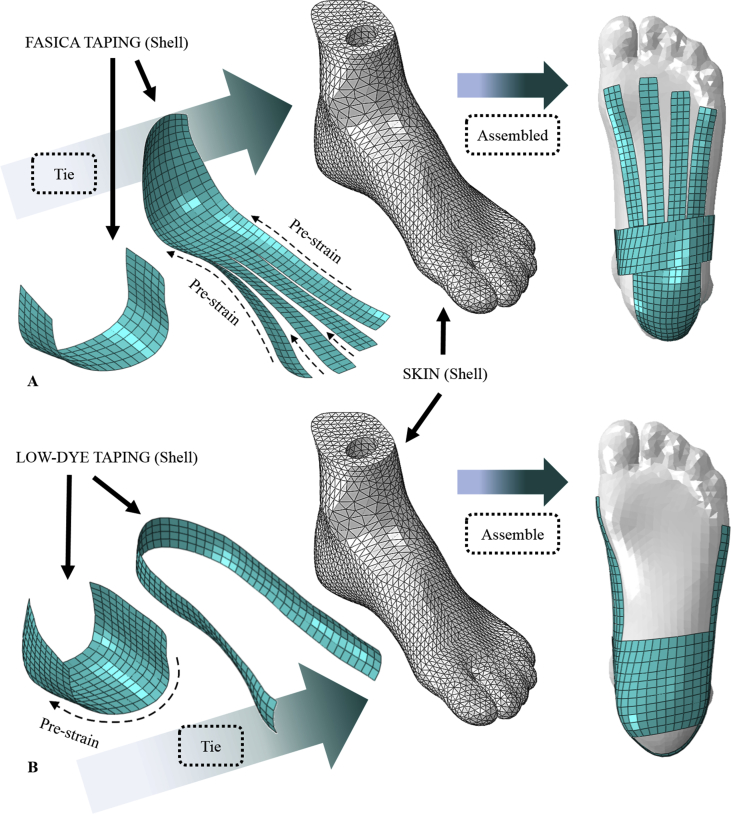
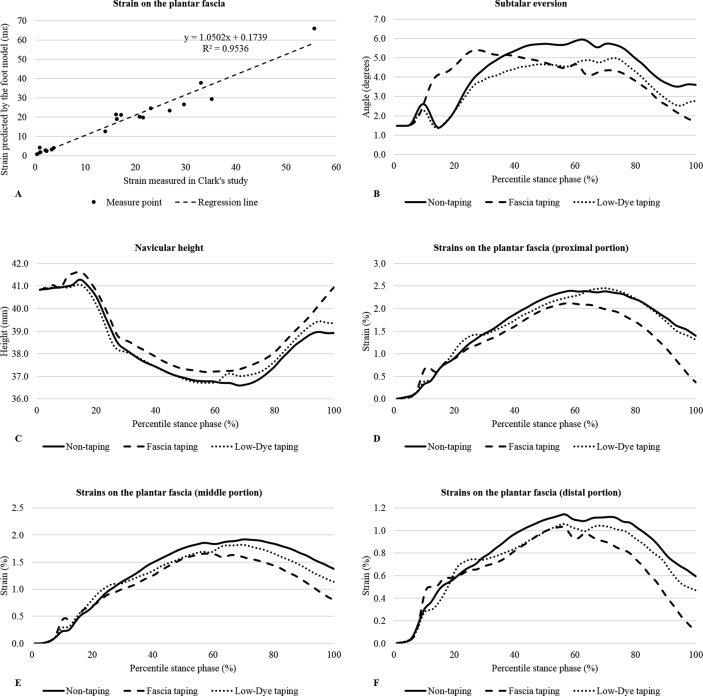
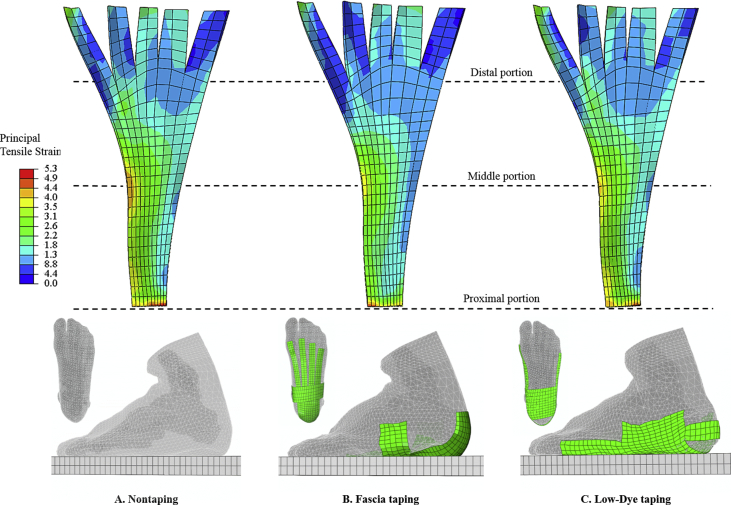
Methods: A finite element foot model was modified from a previous version to fit the study's purpose. The model featured twenty bones, bulk soft tissue, foot muscles, ligaments/tendons, and a solid part representing the plantar fascia. A runner performed several running trials under one untaped condition and two taped conditions-Low-Dye taping and Fascia taping, which were implemented by a physiotherapist using the Kinesio tapes. The captured motion data were processed to drive a scaled musculoskeletal model and calculate segmental kinematics, foot muscle force, and joint reaction force. These variables were then input as the boundary/loading conditions for finite element analyses of running. The principal tensile strain on the plantar fascia, subtalar eversion, and navicular height during the stance phase were averaged across five trials of each condition and compared using Friedman's test.
Results: Maximal subtalar eversion did not differ among conditions (p = 0.449). Fascia taping significantly reduced maximal strains on the fascia band (p = 0.034, Kendall's W = 0.64-0.76) and increased the navicular height (p = 0.013, Kendall's W = 0.84) compared with nontaping. There were no significant differences in all outcome variables between Low-Dye taping and nontaping (p = 0.173-0.618).
Conclusion: From a mechanical point of view, our study provided quantitative evidence to support the application of taping treatments for overstrained plantar fascia. The untensed fascia band by Fascia taping could be a potential indicator of pain relief for the runners. However, a prospective study targeting the patient population would be needed to address the point.
The translational potential of this article: The study quantified the loading status of the plantar fascia during running and provided mechanical evidence to support the usage of taping as a mean to reduce fascial strain, thus possibly controlling injury risks for the runners. The results of the study also highlighted the importance of selecting specific taping methods based on individuals' needs.
Keywords: Athletic tape; Biomechanics; Finite element analysis; Plantar fascia; Running.
© 2019 The Authors.
Figures

References
-
- Jamali B., Walker M., Hoke B., Echternach J. Windlass taping technique for symptomatic relief of plantar fasciitis. J Sport Rehabil. 2004;13:228–243.
-
- Riddle D.L., Pulisic M., Pidcoe P., Johnson R.E. Risk factors for Plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003;85-A 872–7. - PubMed
-
- Buchbinder R. Clinical practice. Plantar fasciitis. N Engl J Med. 2004;350:2159–2166. - PubMed
-
- Tong K.B., Furia J. Economic burden of plantar fasciitis treatment in the United States. Am J Orthoped. 2010;39:227–231. - PubMed
-
- Wearing S.C., Smeathers J.E., Urry S.R., Hennig E.M., Hills A.P. The pathomechanics of plantar fasciitis. Sport Med. 2006;36:585–611. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
