Frontal Bone Fractures and Frontal Sinus Injuries: Treatment Paradigms
- PMID: 31909005
- PMCID: PMC6933972
- DOI: 10.4103/ams.ams_151_19
Frontal Bone Fractures and Frontal Sinus Injuries: Treatment Paradigms
Abstract
Background: Timely, expeditious and appropriate management of Frontal bone fractures and associated Frontal Sinus (FS) injuries are both crucial as well as challenging. Treatment options vary considerably, depending upon the nature, extent and severity of these injuries as well as operator skill, expertise and experience. In cases of posterior table fractures of the Frontal Sinus, literature reports have in general, propounded direct visualization and exploration of the sinus via a bifrontal craniotomy, followed by sinus cranialization.
Aims and objectives: To review the standard protocols of management of Frontal bone fractures and Frontal Sinus injuries. To assess the efficacy of a more conservative approach in the management of outer and inner table fractures of the FS.
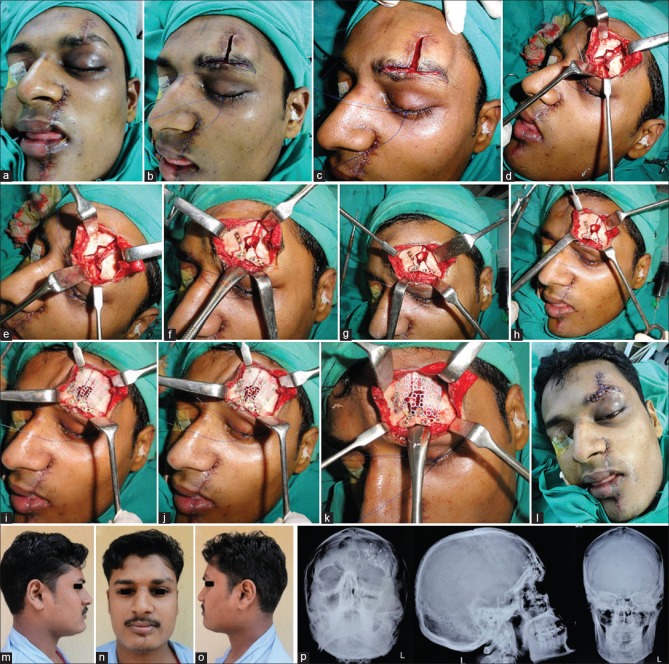
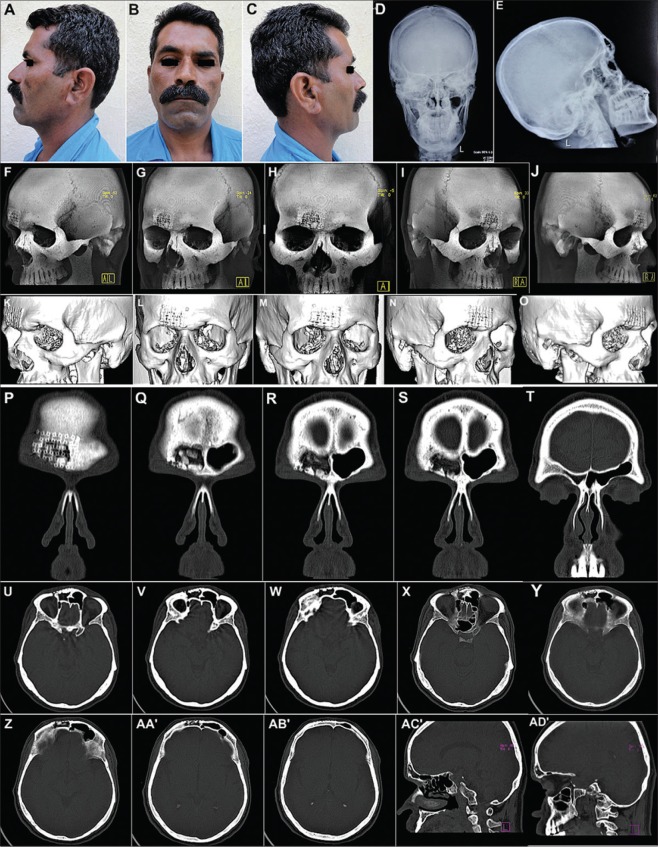
Materials and methods: Contemporary and evolving management protocols and changing treatment paradigms of different types and severities of frontal bone fractures and frontal sinus injuries, have been presented in this case series. A useful Treatment Algorithm has been proposed to efficiently and effectively manage these injuries.
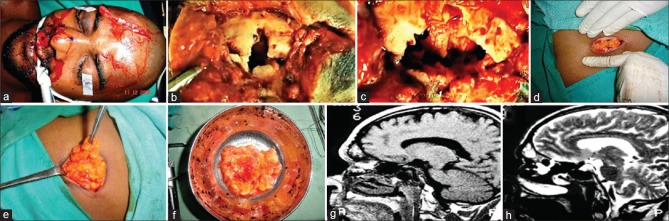
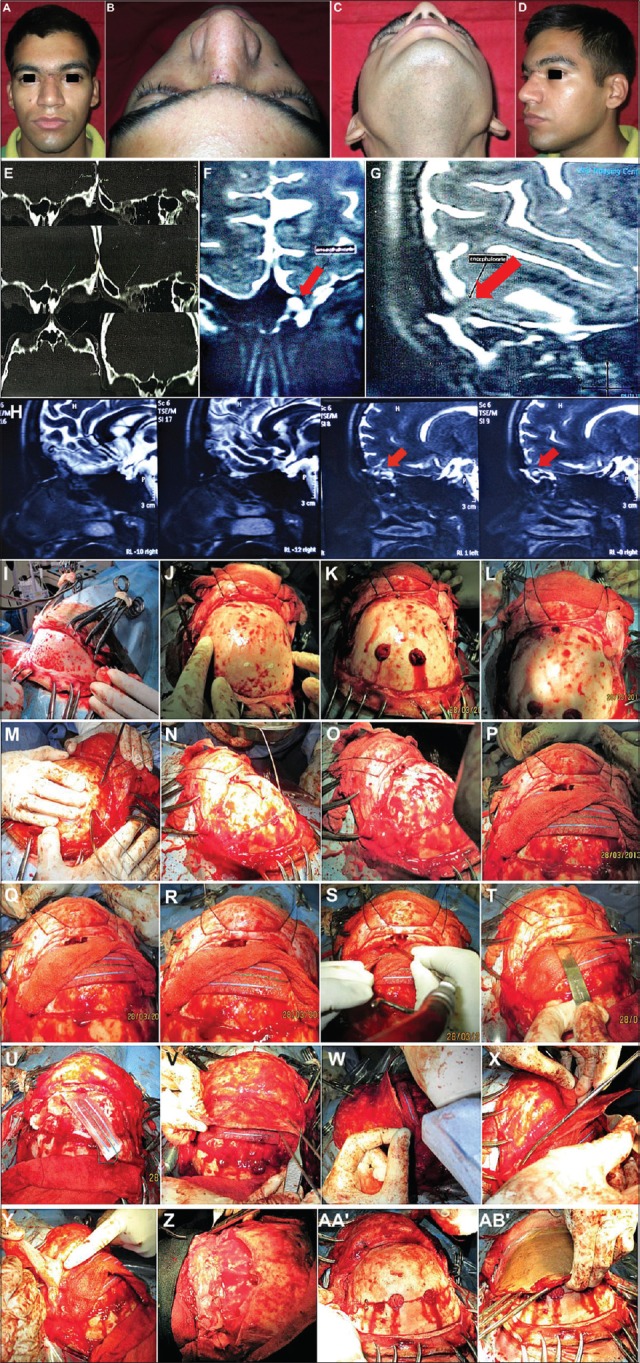
Results: In the present case series, effective and satisfactory results could be achieved in cases of significantly displaced inner and outer table fractures of the Frontal sinus by a more conservative protocol comprising of open reduction and internal fixation carried out via the existing scar of injury, without having to resort to the more radical intracranial approach and sinus cranialization. Nevertheless, presence of complicating factors such as cerebrospinal fluid rhinorrhea, evidence of meningitis or the development of encephalomeningocoeles necessitated the standard protocol of sinus exploration and its cranialization or obliteration.
Conclusion: Management protocols of Frontal Sinus injuries vary, based on aspects such as the timing of presentation and intervention, degree of injury sustained, concomitant associated Craniomaxillofacial injuries present, presence of complicating factors or Secondary/Residual deformities & Functional debility, and need to be decided upon on a case to case basis.
Keywords: Anterior and posterior table fractures of frontal sinus; frontal bone; frontal sinus; frontal sinus cranialization; frontal sinus obliteration; nasofrontal duct; nasofrontal outflow tract; onlay grafting.
Copyright: © 2019 Annals of Maxillofacial Surgery.
Conflict of interest statement
There are no conflicts of interest.
Figures







References
-
- Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D, et al. A retrospective analysis of facial fracture etiologies. Ann Plast Surg. 2008;60:398–403. - PubMed
-
- Strong EB, Pahlavan N, Saito D. Frontal sinus fractures: A 28-year retrospective review. Otolaryngol Head Neck Surg. 2006;135:774–9. - PubMed
-
- Friedman JA, Ebersold MJ, Quast LM. Persistent posttraumatic cerebrospinal fluid leakage. Neurosurg Focus. 2000;9:e1. - PubMed
-
- El Khatib K, Danino A, Malka G. The frontal sinus: A culprit or a victim? A review of 40 cases. J Craniomaxillofac Surg. 2004;32:314–7. - PubMed
-
- Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Incidence and aetiology. J Craniomaxillofac Surg. 2014;42:705–10. - PubMed