Bone Cements in Depressed Frontal Bone Fractures
- PMID: 31909025
- PMCID: PMC6933973
- DOI: 10.4103/ams.ams_155_19
Bone Cements in Depressed Frontal Bone Fractures
Abstract
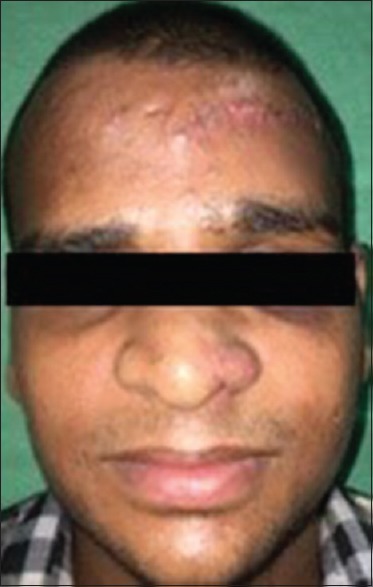
Skull fractures can be classified into four major types; linear, depressed, diastatic, and basilar. Of these, a depressed skull fracture presents a high risk of increased intracranial pressure or hemorrhage to the brain. A compound depressed skull fracture results when a laceration over the fracture exposes the internal cranial cavity to the outside environment. Such depressed skull fractures are indicated for elevation if the defect is more than 10 mm and in the presence of brain injury. Frontal bone contour defects result in marked facial deformity which becomes obvious to the observer. Esthetic correction of the depressed frontal bone fracture can be done with autogenous bone grafts or alloplastic materials. Autogenous bone grafts are meant to be the gold standard method of reconstruction, but they harbor the risk of donor-site morbidity. There are various materials available for the reconstruction of depressed frontal bone fractures. This is a case report which illustrates the use of easily injectable, self-setting calcium phosphate bone cement in the correction of a depressed frontal bone fracture measuring approximately 3 cm × 2.5 cm × 1.5 cm.
Keywords: Bone cement; calcium phosphate cements; contour defects; craniofacial trauma; frontal bone; reconstruction.
Copyright: © 2019 Annals of Maxillofacial Surgery.
Conflict of interest statement
There are no conflicts of interest.
Figures






Similar articles
-
Reconstruction of post-traumatic frontal-bone depression using hydroxyapatite cement.Ann Plast Surg. 2004 Mar;52(3):303-8; discussion 309. doi: 10.1097/01.sap.0000105522.32658.2f. Ann Plast Surg. 2004. PMID: 15156987
-
Cranioplasty of Hemispherical Defects Using Calcium Phosphate Cements Along with Titanium Mesh: Our Experience.J Maxillofac Oral Surg. 2015 Dec;14(4):920-4. doi: 10.1007/s12663-015-0776-3. Epub 2015 Mar 21. J Maxillofac Oral Surg. 2015. PMID: 26604464 Free PMC article.
-
Reconstruction of depressed skull fracture in school patients. Technique description.Cir Cir. 2022;90(5):627-631. doi: 10.24875/CIRU.21000016. Cir Cir. 2022. PMID: 36327480 English.
-
Complications after craniofacial reconstruction with calcium phosphate cements: a case report and review of the literature.J Korean Assoc Oral Maxillofac Surg. 2018 Oct;44(5):207-211. doi: 10.5125/jkaoms.2018.44.5.207. Epub 2018 Oct 26. J Korean Assoc Oral Maxillofac Surg. 2018. PMID: 30402411 Free PMC article. Review.
-
Art of replacing craniofacial bone defects.Yonsei Med J. 2000 Dec;41(6):756-65. doi: 10.3349/ymj.2000.41.6.756. Yonsei Med J. 2000. PMID: 11204826 Review.
Cited by
-
How Partial Skull Defect Affects Vulnerability of the Skull in Traumatic Situations: A Biomechanical Study.Eplasty. 2022 May 12;22:e13. eCollection 2022. Eplasty. 2022. PMID: 35811644 Free PMC article.
-
Primary reconstruction of depressed frontal bone fracture including cranialization of frontal sinus and repair of forehead skin: a case report and literature review.AME Case Rep. 2025 Jul 11;9:92. doi: 10.21037/acr-2025-85. eCollection 2025. AME Case Rep. 2025. PMID: 40761200 Free PMC article.
-
Hardness of Artificial Bone and Vulnerability of Reconstructed Skull-A Biomechanical Study.Eplasty. 2022 Sep 15;22:e41. eCollection 2022. Eplasty. 2022. PMID: 37035411 Free PMC article.
References
-
- Pappachan B, Alexander M. Correlating facial fractures and cranial injuries. J Oral Maxillofac Surg. 2006;64:1023–9. - PubMed
-
- Hannink G, Wolke JG, Schreurs BW, Buma P. In vivo behavior of a novel injectable calcium phosphate cement compared with two other commercially available calcium phosphate cements. J Biomed Mater Res B Appl Biomater. 2008;85:478–88. - PubMed
-
- Garg RK, Afifi AM, Gassner J, Hartman MJ, Leverson G, King TW, et al. A novel classification of frontal bone fractures: The prognostic significance of vertical fracture trajectory and skull base extension. J Plast Reconstr Aesthet Surg. 2015;68:645–53. - PubMed
-
- Gullane PJ, Gilbert RW. Approach to naso-frontal-ethmoidal complex fractures. The Journal of Otolaryngology. 1985;14:132–5. - PubMed