Higher enhanced computed tomography attenuation value of the aorta is a predictor of massive transfusion in blunt trauma patients
- PMID: 31910504
- PMCID: PMC6952635
- DOI: 10.15441/ceem.18.090
Higher enhanced computed tomography attenuation value of the aorta is a predictor of massive transfusion in blunt trauma patients
Abstract
Objective: Several scoring systems have been developed to identify patients who require massive transfusion (MT) after major trauma to improve survival. The primary goal of this study was to investigate the usefulness of enhanced computed tomography attenuation values (CTAVs) of major vessels to determine the need for MT in patients with major blunt trauma.
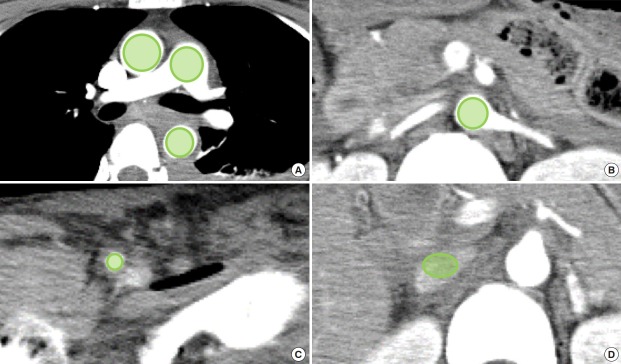
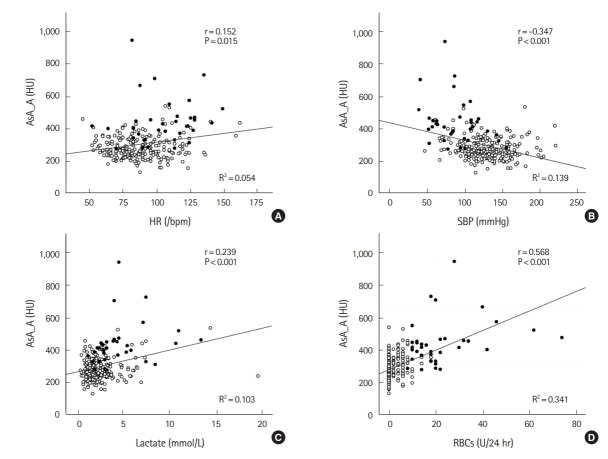
Methods: This single-center retrospective cohort study evaluated patients aged 16 years or older who underwent contrast-enhanced computed tomography scan of the torso after major blunt trauma. The CTAVs of six major vessel points in both the arterial and portal venous phases at initial computed tomography examination were assessed and compared between the MT and the no MT group. The capability of enhanced CTAVs to predict the necessity for MT was estimated based on the area under the receiver operating characteristic curve.
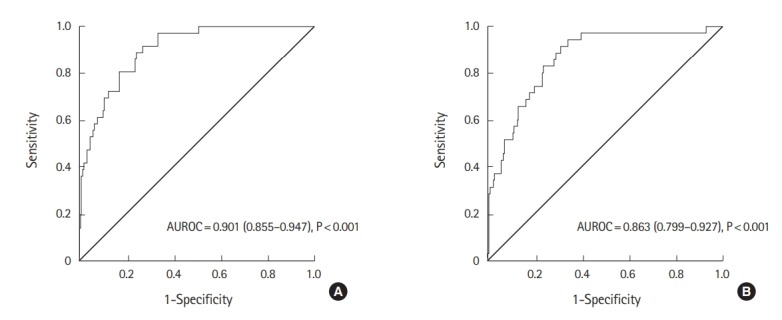
Results: Of the 254 eligible patients, 36 (14%) were in the MT group. Patients in the MT group had significantly higher CTAVs at all sites except the inferior vena cava in both the arterial and portal venous phases than that in the no MT group. The descending aorta in the arterial phase had the highest accuracy for predicting MT, with an AUROC of 0.901 (95% confidence interval, 0.855 to 0.947; P<0.001).
Conclusion: Initial elevation of enhanced CTAV of the aorta is a predictor for the need for MT. A higher CTAV of the aorta should alert the trauma surgeon or emergency physician to activate their MT protocol.
Keywords: Computed tomography attenuated value; Massive transfusion; Wounds and injuries.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Initial inferior vena cava diameter predicts massive transfusion requirements in blunt trauma patients: A retrospective cohort study.Am J Emerg Med. 2018 Jul;36(7):1155-1159. doi: 10.1016/j.ajem.2017.11.049. Epub 2017 Nov 21. Am J Emerg Med. 2018. PMID: 29174329
-
Blunt Trauma Massive Transfusion (B-MaT) Score: A Novel Scoring Tool.J Surg Res. 2022 Feb;270:321-326. doi: 10.1016/j.jss.2021.09.034. Epub 2021 Oct 29. J Surg Res. 2022. PMID: 34731729
-
A simple predictive formula for the blood requirement in patients with high-energy blunt injuries transferred within one hour post-trauma.Acute Med Surg. 2014 Oct 20;2(2):82-91. doi: 10.1002/ams2.74. eCollection 2015 Apr. Acute Med Surg. 2014. PMID: 29123699 Free PMC article.
-
Fibrinogen level on admission is a predictor for massive transfusion in patients with severe blunt trauma: Analyses of a retrospective multicentre observational study.Injury. 2017 Mar;48(3):674-679. doi: 10.1016/j.injury.2017.01.031. Epub 2017 Jan 16. Injury. 2017. PMID: 28122682
-
Fibrinogen and base excess levels as predictive markers of the need for massive blood transfusion after blunt trauma.Surg Today. 2016 Jul;46(7):774-9. doi: 10.1007/s00595-015-1263-7. Epub 2015 Nov 3. Surg Today. 2016. PMID: 26530517 Free PMC article.
Cited by
-
Hemolysis Control in the Emergency Department by Interventional Blood Sampling.J Pers Med. 2023 Apr 10;13(4):651. doi: 10.3390/jpm13040651. J Pers Med. 2023. PMID: 37109037 Free PMC article.
References
-
- Dutton RP, Stansbury LG, Leone S, Kramer E, Hess JR, Scalea TM. Trauma mortality in mature trauma systems: are we doing better? An analysis of trauma mortality patterns, 1997-2008. J Trauma. 2010;69:620–6. - PubMed
-
- Huber-Wagner S, Lefering R, Qvick LM, et al. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet. 2009;373:1455–61. - PubMed
-
- Hoyt DB, Bulger EM, Knudson MM, et al. Death in the operating room: an analysis of a multi-center experience. J Trauma. 1994;37:426–32. - PubMed
-
- Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62:307–10. - PubMed
LinkOut - more resources
Full Text Sources