

Computerized clinical decision support system for diabetes in primary care does not improve quality of care: a cluster-randomized controlled trial
- PMID: 31910877
- PMCID: PMC6947861
- DOI: 10.1186/s13012-019-0955-6
Computerized clinical decision support system for diabetes in primary care does not improve quality of care: a cluster-randomized controlled trial
Abstract
Background: The EBMeDS system is the computerized clinical decision support (CCDS) system of EBPNet, a national computerized point-of-care information service in Belgium. There is no clear evidence of more complex CCDS systems to manage chronic diseases in primary care practices (PCPs). The objective of this study was to assess the effectiveness of EBMeDS use in improving diabetes care.
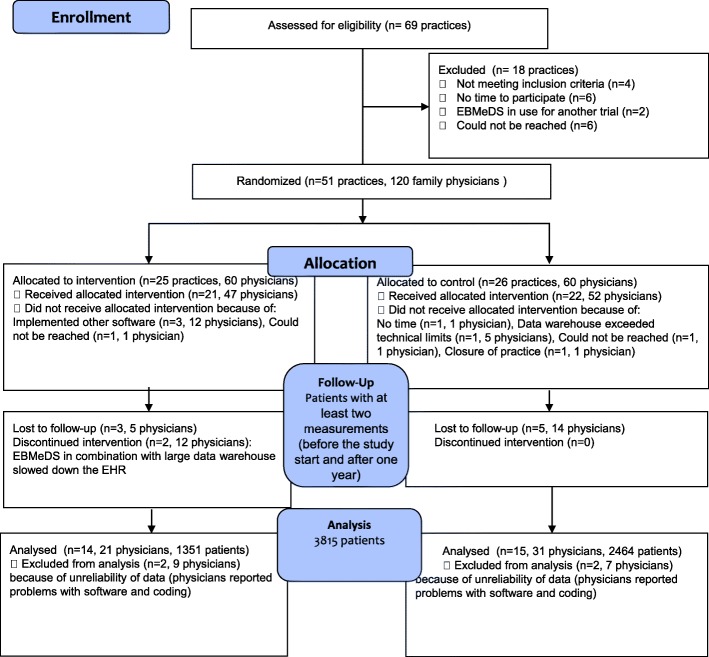
Methods: A cluster-randomized trial with before-and-after measurements was performed in Belgian PCPs over 1 year, from May 2017 to May 2018. We randomly assigned 51 practices to either the intervention group (IG), to receive the EBMeDS system, or to the control group (CG), to receive usual care. Primary and secondary outcomes were the 1-year pre- to post-implementation change in HbA1c, LDL cholesterol, and systolic and diastolic blood pressure. Composite patient and process scores were calculated. A process evaluation was added to the analysis. Results were analyzed at 6 and 12 months. Linear mixed models and logistic regression models based on generalized estimating equations were used where appropriate.
Results: Of the 51 PCPs that were enrolled and randomly assigned (26 PCPs in the CG and 25 in the IG), 29 practices (3815 patients) were analyzed in the study: 2464 patients in the CG and 1351 patients in the IG. No change differences existed between groups in primary or secondary outcomes. Change difference between CG and IG after 1-year follow-up was - 0.09 (95% CI - 0.18; 0.01, p-value = 0.06) for HbA1c; 1.76 (95% CI - 0.46; 3.98, p-value = 0.12) for LDL cholesterol; and 0.13 (95% CI - 0.91; 1.16, p-value = 0.81) and 0.12 (95% CI - 1.25;1.49, p-value = 0.86) for systolic and diastolic blood pressure respectively. The odds ratio of the IG versus the CG for the probability of no worsening and improvement was 1.09 (95% CI 0.73; 1.63, p-value = 0.67) for the process composite score and 0.74 (95% CI 0.49; 1.12, p-value = 0.16) for the composite patient score. All but one physician was satisfied with the EBMeDS system.
Conclusions: The CCDS system EBMeDS did not improve diabetes care in Belgian primary care. The lack of improvement was mainly caused by imperfections in the organizational context of Belgian primary care for chronic disease management and shortcomings in the system requirements for the correct use of the EBMeDS system (e.g., complete structured records). These shortcomings probably caused low-use rates of the system.
Trial registration: ClinicalTrials.gov, NCT01830569, Registered 12 April 2013.
Keywords: Decision support systems, clinical; Diabetes Mellitus; Electronic Health Records; Primary Health Care; Randomized Controlled Trial; Reminder systems.
Conflict of interest statement
AL, BA, and DR have no competing interests. AH and SVdV were former salaried editors of EBPNet, the organization responsible for the implementation of EBMeDS in Belgian family medicine. ND is a project leader of EBMeDS in Belgium. IK is a salaried employee of Duodecim Medical Publications Ltd., the company that develops and licenses the EBMeDS decision support service.
References
-
- Haynes RB, Wilczynski NL, The Computerized Clinical Decision Support System (CCDSS) Systematic Review Team Effects of Computerized Clinical Decision Support Systems on Practitioner Performance and patient outcomes: Methods of a decision-maker-researcher partnership systematic review. Implement Sci. 2010;5:12. doi: 10.1186/1748-5908-5-12. - DOI - PMC - PubMed
-
- Nieuwlaat R, Connolly SJ, Mackay JA, Weise-Kelly L, Navarro T, Wilczynski NL, The CCDSS Systematic Review Team. Computerized clinical decision support systems for therapeutic drug monitoring and dosing: a decision-maker-researcher partnership systematic review. Implement Sci. 2011;6:90. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
