

Tumor Analyses Reveal Squamous Transformation and Off-Target Alterations As Early Resistance Mechanisms to First-line Osimertinib in EGFR-Mutant Lung Cancer
- PMID: 31911548
- PMCID: PMC7448565
- DOI: 10.1158/1078-0432.CCR-19-3563
Tumor Analyses Reveal Squamous Transformation and Off-Target Alterations As Early Resistance Mechanisms to First-line Osimertinib in EGFR-Mutant Lung Cancer
Abstract
Purpose: Patterns of resistance to first-line osimertinib are not well-established and have primarily been evaluated using plasma assays, which cannot detect histologic transformation and have differential sensitivity for copy number changes and chromosomal rearrangements.
Experimental design: To characterize mechanisms of resistance to osimertinib, patients with metastatic EGFR-mutant lung cancers who received osimertinib at Memorial Sloan Kettering Cancer Center and had next-generation sequencing performed on tumor tissue before osimertinib initiation and after progression were identified.
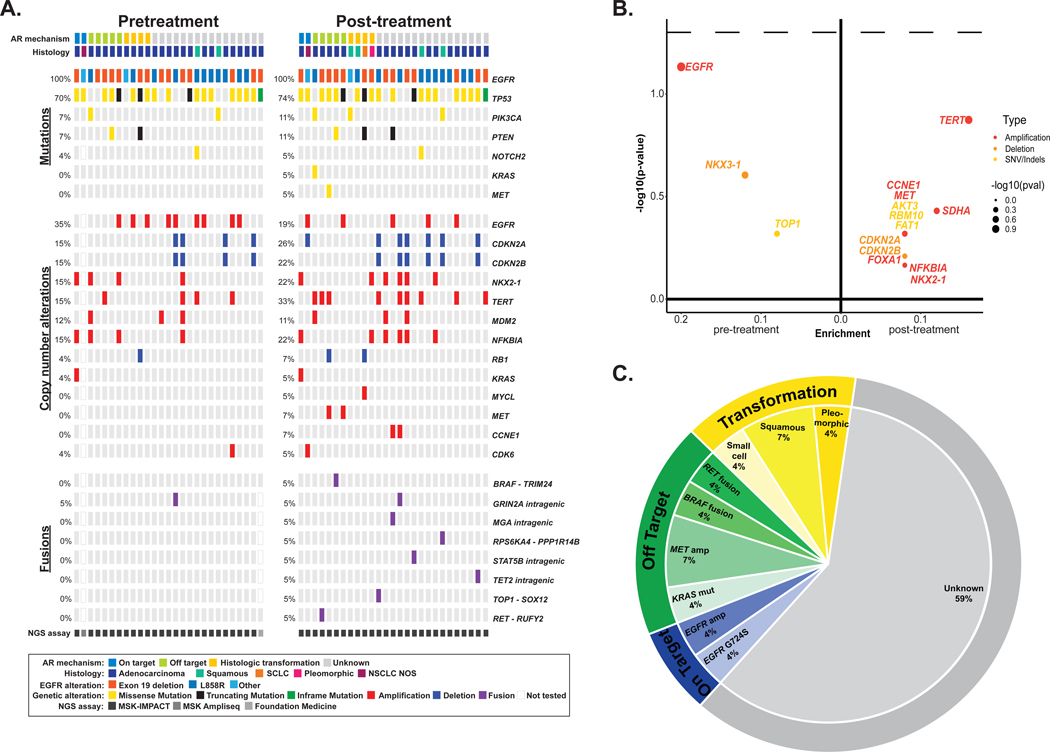
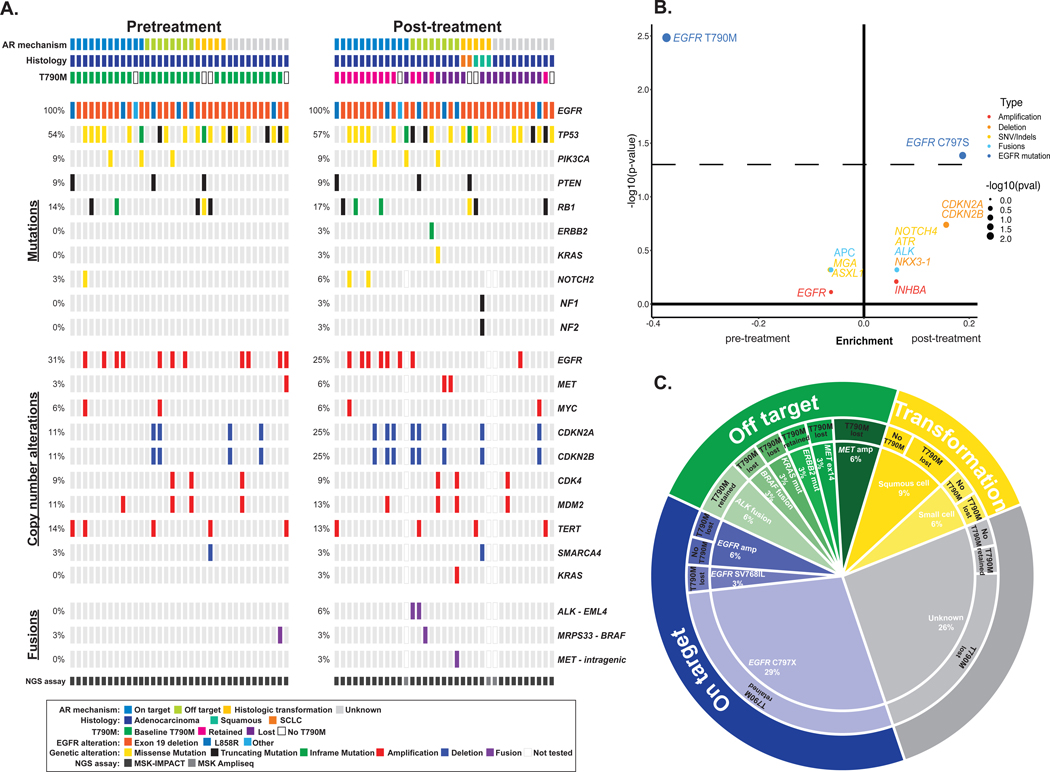
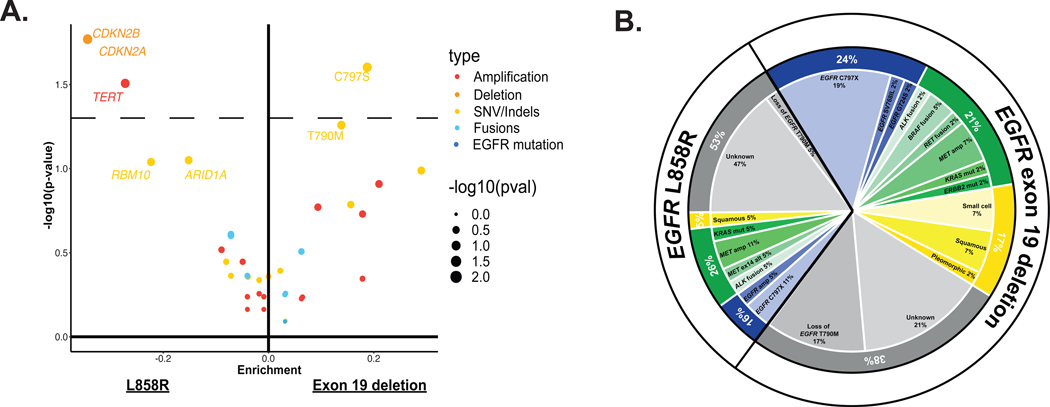
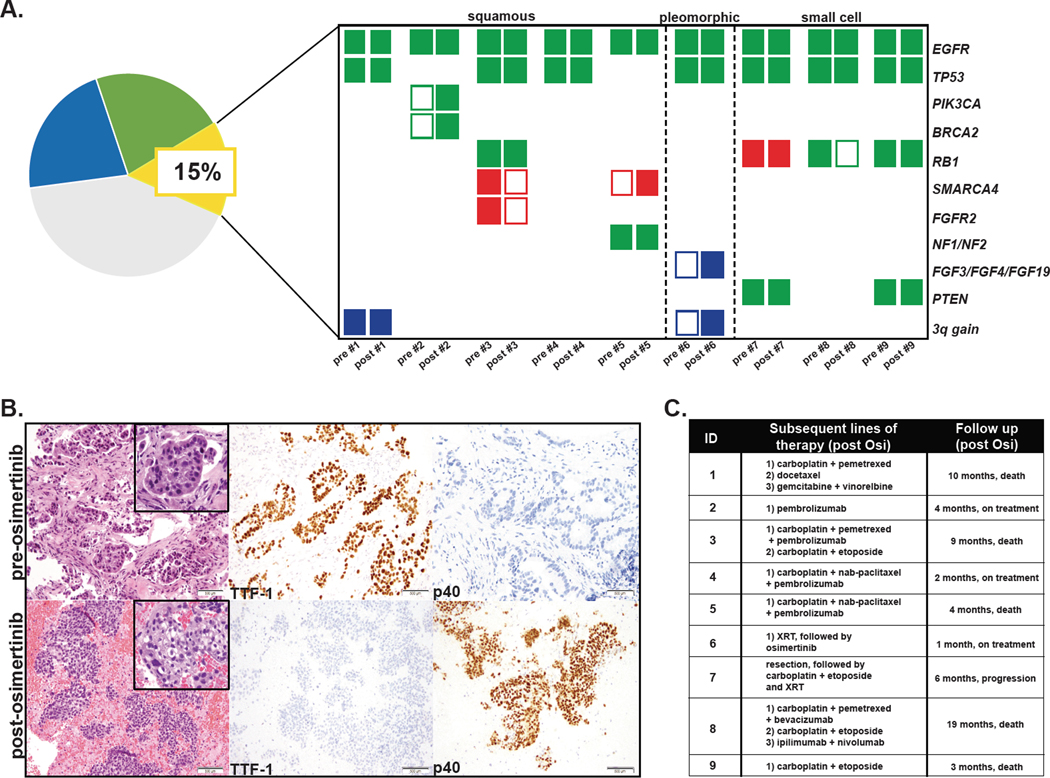
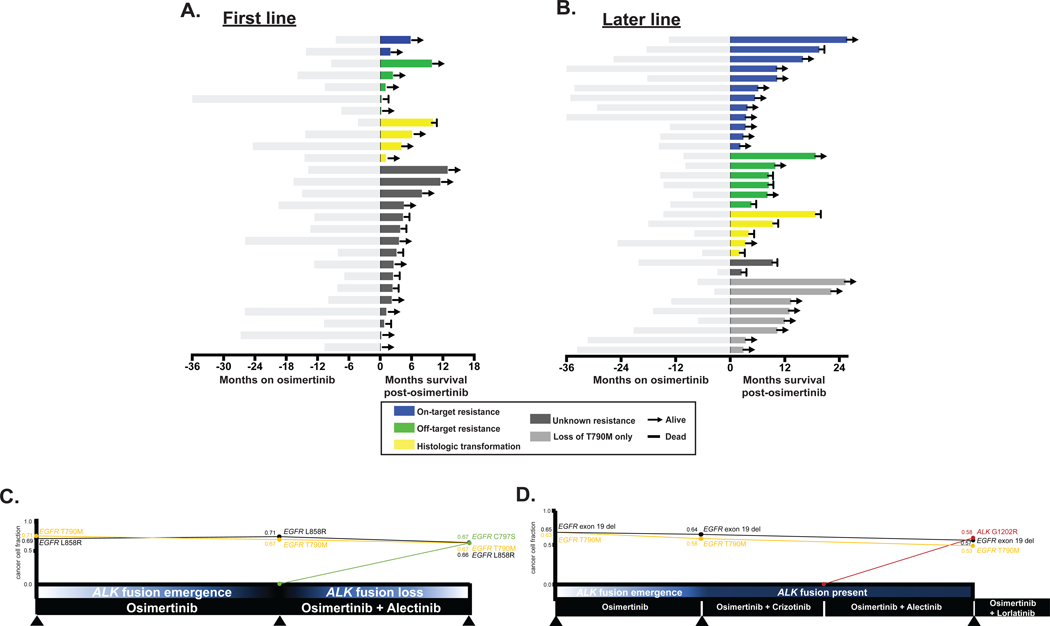
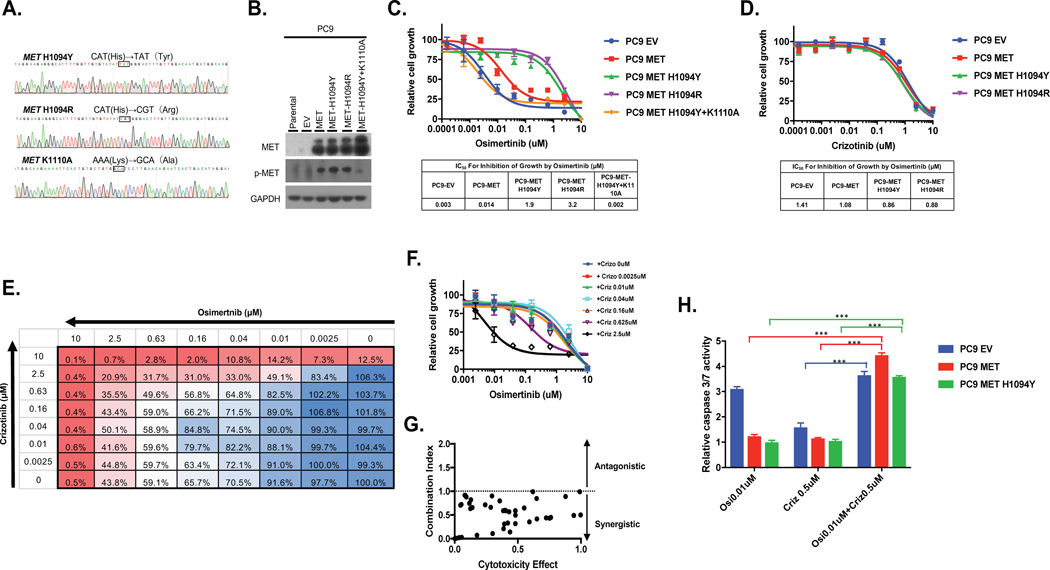
Results: Among 62 patients who met eligibility criteria, histologic transformation, primarily squamous transformation, was identified in 15% of first-line osimertinib cases and 14% of later-line cases. Nineteen percent (5/27) of patients treated with first-line osimertinib had off-target genetic resistance (2 MET amplification, 1 KRAS mutation, 1 RET fusion, and 1 BRAF fusion) whereas 4% (1/27) had an acquired EGFR mutation (EGFR G724S). Patients with squamous transformation exhibited considerable genomic complexity; acquired PIK3CA mutation, chromosome 3q amplification, and FGF amplification were all seen. Patients with transformation had shorter time on osimertinib and shorter survival compared with patients with on-target resistance. Initial EGFR sensitizing mutation, time on osimertinib treatment, and line of therapy also influenced resistance mechanism that emerged. The compound mutation EGFR S768 + V769L and the mutation MET H1094Y were identified and validated as resistance mechanisms with potential treatment options.
Conclusions: Histologic transformation and other off-target molecular alterations are frequent early emerging resistance mechanisms to osimertinib and are associated with poor clinical outcomes.See related commentary by Piotrowska and Hata, p. 2441.
©2020 American Association for Cancer Research.
Figures
Comment in
-
Resistance to First-line Osimertinib in EGFR-mutant NSCLC: Tissue is the Issue.Clin Cancer Res. 2020 Jun 1;26(11):2441-2443. doi: 10.1158/1078-0432.CCR-20-0097. Epub 2020 Mar 26. Clin Cancer Res. 2020. PMID: 32217611
Comment on
-
Resistance to First-line Osimertinib in EGFR-mutant NSCLC: Tissue is the Issue.Clin Cancer Res. 2020 Jun 1;26(11):2441-2443. doi: 10.1158/1078-0432.CCR-20-0097. Epub 2020 Mar 26. Clin Cancer Res. 2020. PMID: 32217611
References
-
- Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clinical cancer research : an official journal of the American Association for Cancer Research 2013;19(8):2240–7 doi 10.1158/1078-0432.ccr-12-2246. - DOI - PMC - PubMed
-
- Piotrowska Z, Isozaki H, Lennerz JK, Gainor JF, Lennes IT, Zhu VW, et al. Landscape of acquired resistance to osimertinib in EGFR-mutant NSCLC and clinical validation of combined EGFR and RET inhibition with osimertinib and BLU-667 for acquired RET fusion. Cancer discovery 2018;8(12):1529–39 doi 10.1158/2159-8290.Cd-18-1022. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
