

The neurobiology of treatment-resistant schizophrenia: paths to antipsychotic resistance and a roadmap for future research
- PMID: 31911624
- PMCID: PMC6946650
- DOI: 10.1038/s41537-019-0090-z
The neurobiology of treatment-resistant schizophrenia: paths to antipsychotic resistance and a roadmap for future research
Abstract
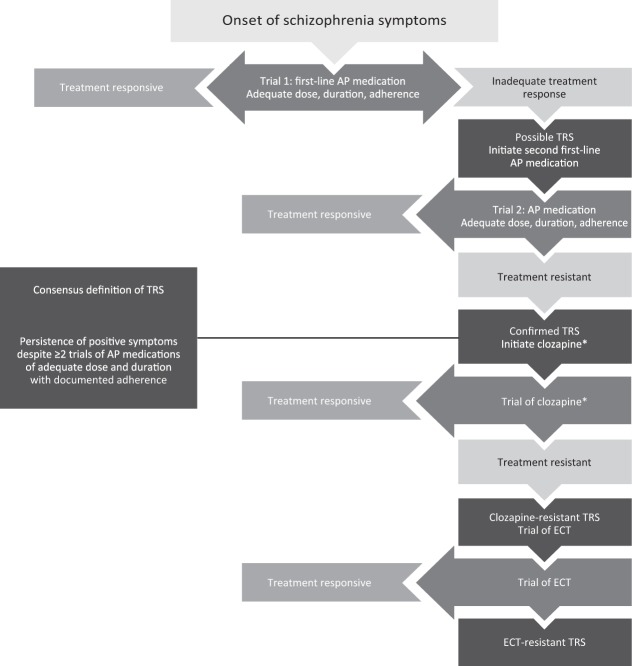
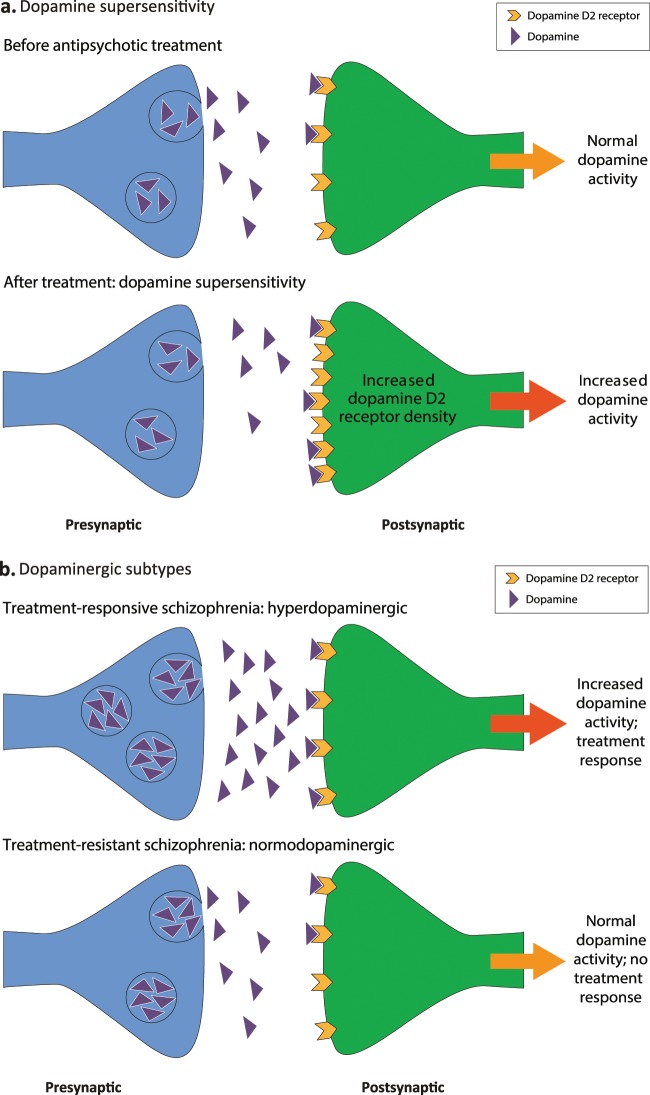
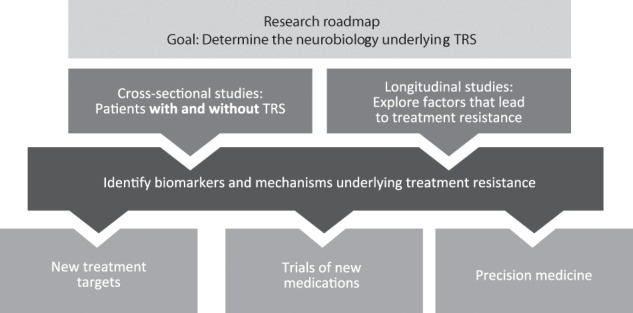
Treatment-resistant schizophrenia (TRS), the persistence of positive symptoms despite ≥2 trials of adequate dose and duration of antipsychotic medication with documented adherence, is a serious clinical problem with heterogeneous presentations. TRS can vary in its onset (at the first episode of psychosis or upon relapse), in its severity, and in the response to subsequent therapeutic interventions (i.e., clozapine, electroconvulsive therapy). The heterogeneity of TRS indicates that the underlying neurobiology of TRS may differ not only from treatment-responsive schizophrenia but also among patients with TRS. Several hypotheses have been proposed for the neurobiological mechanisms underlying TRS, including dopamine supersensitivity, hyperdopaminergic and normodopaminergic subtypes, glutamate dysregulation, inflammation and oxidative stress, and serotonin dysregulation. Research supporting these hypotheses is limited in part by variations in the criteria used to define TRS, as well as by the biological and clinical heterogeneity of TRS. Clinical trial designs for new treatments should be informed by this heterogeneity, and further clinical research is needed to more clearly understand the underlying neurobiology of TRS and to optimize treatment for patients with TRS.
Conflict of interest statement
Dr Potkin has been a consultant and/or advisor to or has received honoraria from Alkermes, Allergan, Gerson Lehrman Group, Lundbeck, Medscape, Merck, Otsuka, Pfizer, Sunovion, Takeda, Teva, Toyama Chemical Co, and Vanda Pharmaceuticals and has received grant support from Allergan, Otsuka, Lundbeck, Takeda, the University of California San Diego, and the University of Southern California. Dr Kane has been a consultant and/or advisor to or has received honoraria from Alkermes, Allergan, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, Medscape, Neurocrine, Newron, Otsuka, Pfizer, Pierre Fabre, Reviva, Roche, Sunovion, Takeda, and Teva. He has received grant support from Janssen/J&J, Lundbeck, and Otsuka. He is a shareholder of The Vanguard Research Group and LB Pharma. Dr Correll has been a consultant and/or advisor or received honoraria from Alkermes, Allergan, Angelini, Boehringer-Ingelheim, Gerson Lehrman Group, Indivior, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Merck, Neurocrine, Noven, Otsuka, Pfizer, Rovi, Servier, Sunovion, Supernus, Takeda, and Teva. He reports providing expert testimony for Bristol-Myers Squibb, Janssen, and Otsuka and serving on a Data Safety Monitoring Board for Boehringer-Ingelheim, Lundbeck, Rovi, Sumitomo Dainippon, Supernus, and Teva. He received royalties from UpToDate. He received grants from Janssen and Takeda and is a shareholder of LB Pharma. Dr Lindenmayer has been a consultant for Alkermes, Janssen/J&J, Lundbeck, Neurocrine, Newron, and Otsuka, and has received research grant support from Alkermes, Astellas, Avanir, Intracellular, Janssen, Neurocrine, Newron, Roche, and Takeda. Dr Agid has been a consultant and/or advisor to or has received honoraria from Janssen-Ortho (Johnson & Johnson), Otsuka, Lundbeck, Sumitomo Dainippon Pharma (DSP), Mylan Pharmaceuticals, and HLS Therapeutics. He has received grant support from Janssen-Ortho (Johnson & Johnson), Otsuka, Boehringer Ingelheim, and Neurocrine Biosciences. Dr Marder has been a consultant or advisory board member for Allergan, Boehringer Ingelheim, Lundbeck, Neurocrine, Newron, Otsuka, Roche, and Teva, and has received research support from Boehringer Ingelheim, Neurocrine, and Takeda. Dr Olfson has served as a consultant to Lundbeck. Dr Howes has received investigator-initiated research funding from and/or participated in advisory/speaker meetings organized by Angellini, Autifony (grants only), Biogen (non-financial support), Heptares (grants only), Janssen, Lundbeck, Otsuka, Sunovion, Rand (non-financial support), and Roche. Neither Dr Howes nor his family have been employed by or have holdings/a financial stake in any biomedical company.
Figures
References
-
- Lehman, A. F., et al. Practice guideline for the treatment of patients with schizophrenia, second edition. Am. J. Psychiatry161(2 suppl.),1–56 (2004). - PubMed
