

Innovation in Oncology Drug Development
- PMID: 31911803
- PMCID: PMC6930717
- DOI: 10.1155/2019/9683016
Innovation in Oncology Drug Development
Abstract
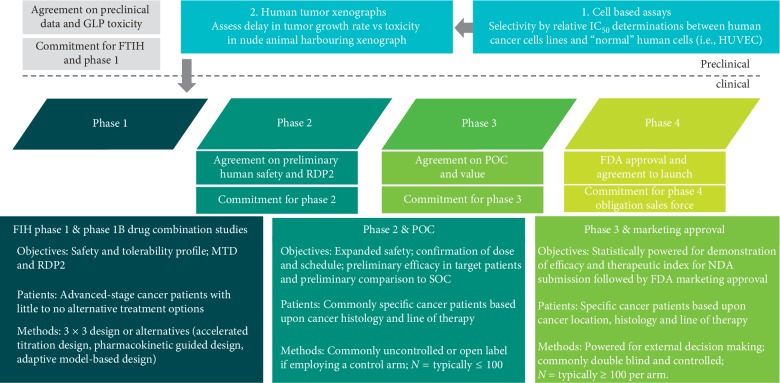
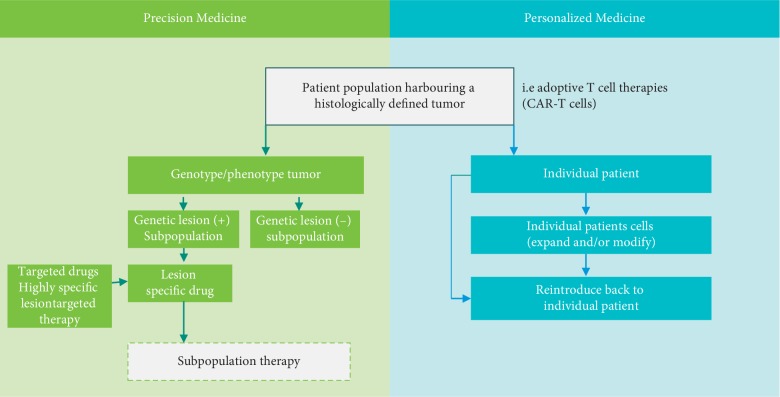
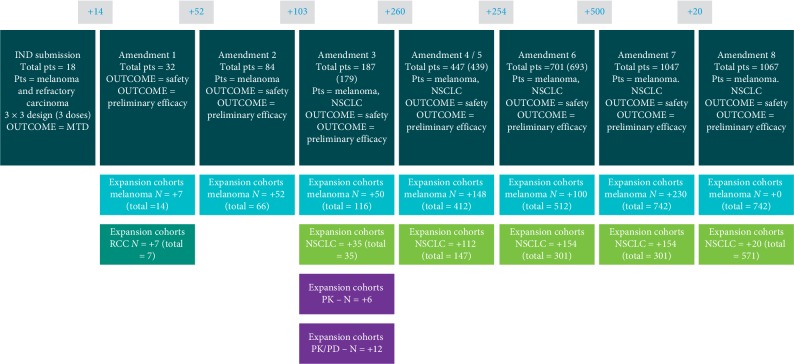
Significant progress has been made in our understanding of the molecular lesions responsible for tumor cells to exhibit uncontrolled growth while circumventing normal mechanisms of apoptosis and their ability to migrate and invade normal tissues while evading recognition and destruction by the immune system. This understanding has enabled the development of therapies specifically targeted to these lesions coupled to innovative treatment regimens to most effectively use these new targeted therapies with precision in selected subpopulations of patients. Innovation at the scientific and clinical levels has been appropriately embraced and supported at the FDA, resulting in regulatory innovation to facilitate and adapt to the Precision Medicine environment.
Copyright © 2019 Matthew Huber and Brian Huber.
Conflict of interest statement
The authors declare that they have no conflicts of interest regarding the publication of this article.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
