

Benefit-to-risk balance of bronchoalveolar lavage in the critically ill. A prospective, multicenter cohort study
- PMID: 31912201
- PMCID: PMC7223716
- DOI: 10.1007/s00134-019-05896-4
Benefit-to-risk balance of bronchoalveolar lavage in the critically ill. A prospective, multicenter cohort study
Abstract
Purpose: To assess the benefit-to-risk balance of bronchoalveolar lavage (BAL) in intensive care unit (ICU) patients.
Methods: In 16 ICUs, we prospectively collected adverse events during or within 24 h after BAL and assessed the BAL input for decision making in consecutive adult patients. The occurrence of a clinical adverse event at least of grade 3, i.e., sufficiently severe to need therapeutic action(s), including modification(s) in respiratory support, defined poor BAL tolerance. The BAL input for decision making was declared satisfactory if it allowed to interrupt or initiate one or several treatments.
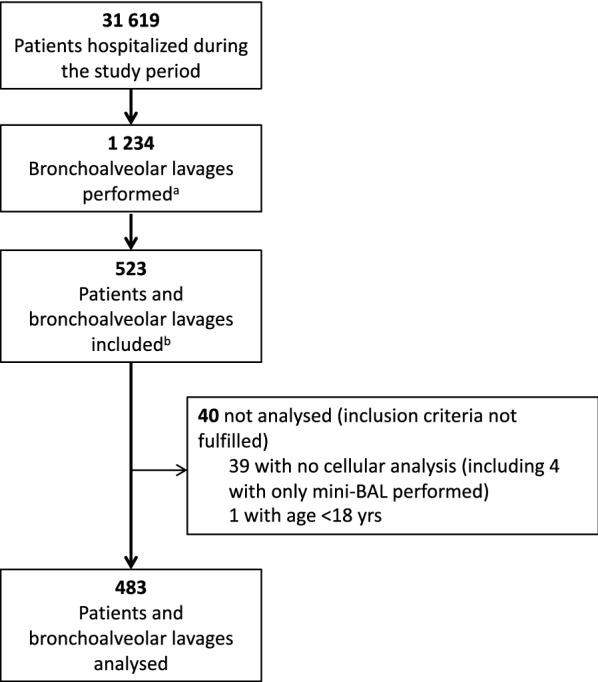
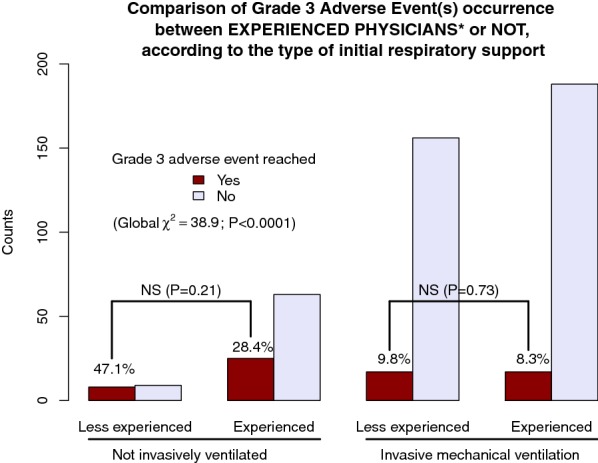
Results: We included 483 BAL in 483 patients [age 63 years (interquartile range (IQR) 53-72); female gender: 162 (33.5%); simplified acute physiology score II: 48 (IQR 37-61); immunosuppression 244 (50.5%)]. BAL was begun in non-intubated patients in 105 (21.7%) cases. Sixty-seven (13.9%) patients reached the grade 3 of adverse event or higher. Logistic regression showed that a BAL performed by a non-experienced physician (non-pulmonologist, or intensivist with less than 10 years in the specialty or less than 50 BAL performed) was the main predictor of poor BAL tolerance in non-intubated patients [OR: 3.57 (95% confidence interval 1.04-12.35); P = 0.04]. A satisfactory BAL input for decision making was observed in 227 (47.0%) cases and was not predictable using logistic regression.
Conclusions: Adverse events related to BAL in ICU patients are not infrequent nor necessarily benign. Our findings call for an extreme caution, when envisaging a BAL in ICU patients and for a mandatory accompaniment of the less experienced physicians.
Keywords: Bronchoalveolar lavage; Fiberoptic bronchoscopy; Intensive care; Multicenter study.
Conflict of interest statement
The authors declare that they have no conflicts of interest in relation to this study.
Figures
Comment in
-
Author's reply.Respir Investig. 2022 Nov;60(6):863-864. doi: 10.1016/j.resinv.2022.07.002. Epub 2022 Aug 20. Respir Investig. 2022. PMID: 35999141 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
