

The influence of time to adrenaline administration in the Paramedic 2 randomised controlled trial
- PMID: 31912202
- PMCID: PMC7067734
- DOI: 10.1007/s00134-019-05836-2
The influence of time to adrenaline administration in the Paramedic 2 randomised controlled trial
Abstract
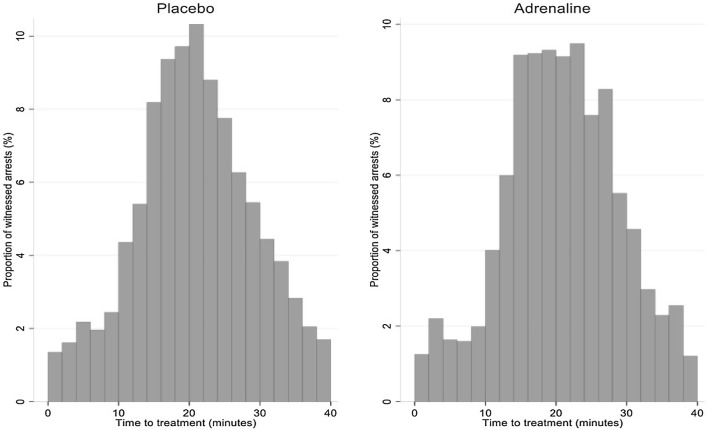
Purpose: To examine the time to drug administration in patients with a witnessed cardiac arrest enrolled in the Pre-Hospital Assessment of the Role of Adrenaline: Measuring the Effectiveness of Drug Administration in Cardiac Arrest (PARAMEDIC2) randomised controlled trial.
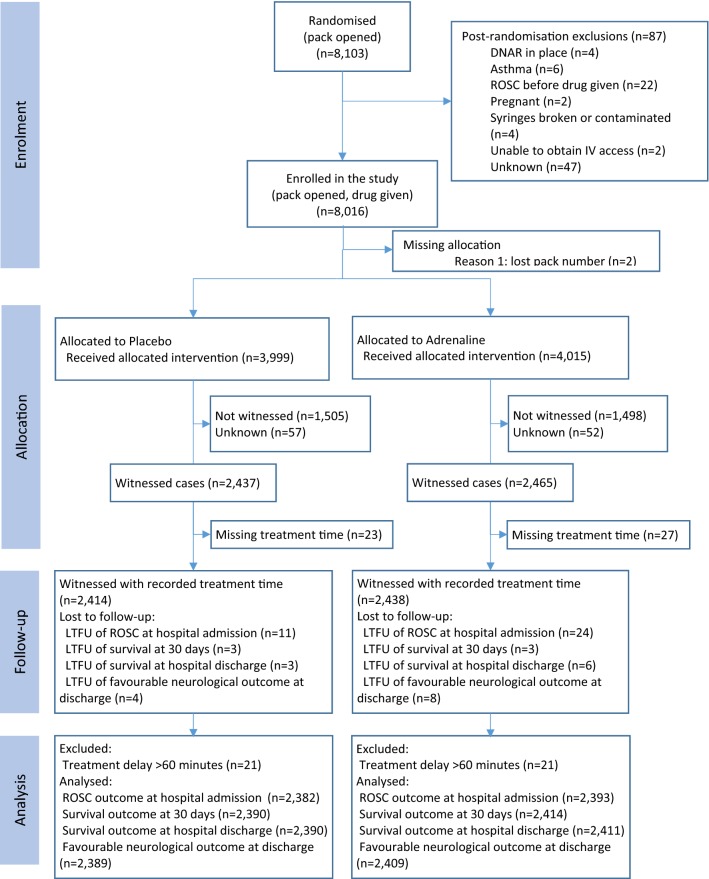
Methods: The PARAMEDIC2 trial was undertaken across 5 NHS ambulance services in England and Wales with randomisation between December 2014 and October 2017. Patients with an out-of-hospital cardiac arrest who were unresponsive to initial resuscitation attempts were randomly assigned to 1 mg intravenous adrenaline or matching placebo according to treatment packs that were identical apart from treatment number. Participants and study staff were masked to treatment allocation.
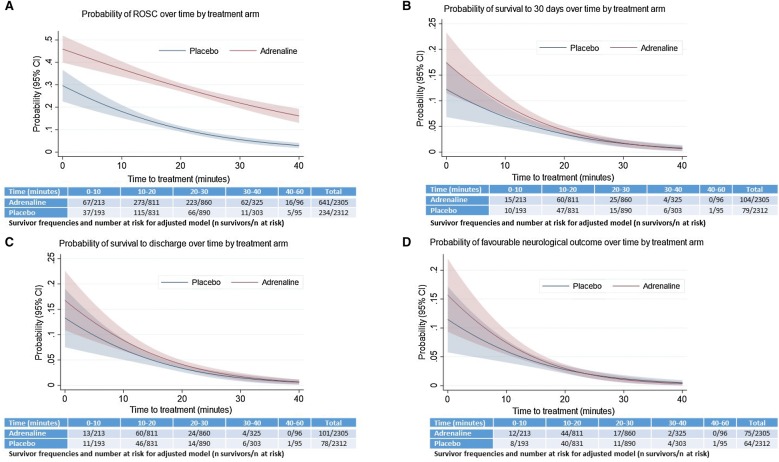
Results: 8016 patients were enrolled, 4902 sustained a witnessed cardiac arrest of whom 2437 received placebo and 2465 received adrenaline. The odds of return of spontaneous circulation decreased in both groups over time but at a greater rate in the placebo arm odds ratio (OR) 0.93 (95% CI 0.92-0.95) compared with the adrenaline arm OR 0.96 (95% CI 0.95-0.97); interaction OR: 1.03, 95% CI 1.01-1.05, p = 0.005. By contrast, although the rate of survival and favourable neurological outcome decreased as time to treatment increased, the rates did not differ between the adrenaline and placebo groups.
Conclusion: The rate of return of spontaneous circulation, survival and favourable neurological outcomes decrease over time. As time to drug treatment increases, adrenaline increases the chances of return of spontaneous circulation. Longer term outcomes were not affected by the time to adrenaline administration. (ISRCTN73485024).
Keywords: Adrenaline; Advanced life support; Cardiac arrest; Drugs; Timing.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures

References
-
- Safar P. Community-wide cardiopulmonary resuscitation. J Iowa Med Soc. 1964;54:629–635. - PubMed
-
- Perkins GD, Ji C, Deakin CD, Quinn T, Nolan JP, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black JJM, Moore F, Fothergill RT, Rees N, O’Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R, Collaborators P. A randomized trial of epinephrine in out-of-hospital cardiac arrest. N Engl J Med. 2018;379(8):711–721. doi: 10.1056/NEJMoa1806842. - DOI - PubMed
-
- Champlin PB. Resuscitation by intracardiac injection of epinephrin chlorid. J Am Med Assoc. 1923;81(3):202–203. doi: 10.1001/jama.1923.02650030026010. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
