

The rise in non-fatal and fatal overdoses involving stimulants with and without opioids in the United States
- PMID: 31912625
- PMCID: PMC11301974
- DOI: 10.1111/add.14878
The rise in non-fatal and fatal overdoses involving stimulants with and without opioids in the United States
Abstract
Aims: To examine trends and recent changes in non-fatal and fatal stimulant overdose rates with and without opioids to improve the descriptive characterization of the US overdose epidemic.
Design: Secondary analysis of non-fatal (2006-16) and fatal (2006-17) drug overdose trends, focusing on the most recent years of data available to examine rate changes by demographics (2015-16 for non-fatal and 2016-17 for fatal).
Setting: Non-fatal drug overdoses from the Healthcare Cost and Utilization Project's Nationwide Emergency Department Sample; drug overdose deaths from the National Vital Statistics System.
Participants/cases: International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) codes for cocaine, psychostimulants and opioids were used to classify non-fatal drug overdoses. Drug overdose deaths were identified using ICD-10 multiple cause-of-death codes for cocaine, psychostimulants, all opioids, heroin and synthetic opioids.
Measurements: Percentage of changes in age-adjusted non-fatal and fatal rates of cocaine and psychostimulant-involved drug overdose with and without opioids.
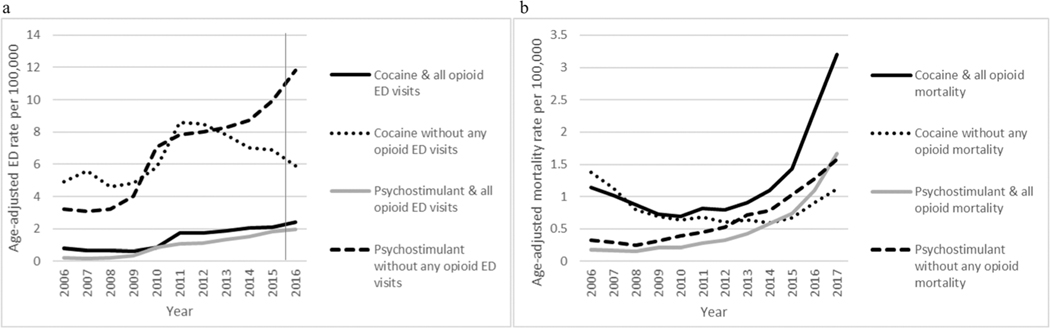
Findings: Overall, cocaine-involved non-fatal overdose rates with an opioid increased from 2006 to 2016 [annual percentage change (APC) = 14.7], while rates without an opioid increased from 2006 to 2012 (APC = 11.3) and then remained stable (APC = -7.5). Psychostimulant-involved non-fatal rates with and without an opioid increased from 2006 to 2016 (APC = 49.9 with opioids; 13.9 without opioids). Cocaine-involved death rates with and without opioids increased from 2014 to 2017 (APC = 46.0 with opioids, 23.6 without opioids). Psychostimulant-involved death rates with opioids increased from 2010 to 2015 (APC = 28.6), with a dramatic increase from 2015 to 2017 (APC = 50.5), while rates without opioids increased from 2008 to 2017 (APC = 22.6). In 2016, 27% of non-fatal cocaine- and 14% of psychostimulant-involved overdoses included a reported opioid; 72.7% of cocaine- and 50.3% of psychostimulant-involved deaths involved an opioid in 2017. From 2015 to 2016, cocaine-involved and psychostimulant-involved non-fatal overdose rates with an opioid increased 17.0 and 5.9%, respectively; cocaine-involved and psychostimulant-involved non-fatal overdoses without opioids decreased 13.6 and increased 18.9%, respectively. Death rates involving stimulants increased with and without opioids from 2016 to 2017 (cocaine with and without opioids = 37.7 and 23.3%; psychostimulants with and without opioids = 52.2 and 23.0%). Death rates involving stimulants with synthetic opioids increased dramatically from 2016 to 2017 (1.3-2.3 per 100 000 for cocaine and 0.3-0.8 for psychostimulants).
Conclusions: While increases in cocaine-involved deaths in the United States from 2006 seem to be driven by opioids, particularly synthetic opioids, increases in non-fatal and fatal overdoses involving psychostimulants are occurring with and without opioids.
Keywords: Cocaine; Opioids; United States; emergency department; overdose; stimulants.
Published 2020. This article is a U.S. Government work and is in the public domain in the USA.
Figures
Comment in
-
Commentary on Hoots et al. (2019): The gap between evidence and policy calls into question the extent of a public health approach to the opioid overdose epidemic.Addiction. 2020 May;115(5):959-960. doi: 10.1111/add.14958. Epub 2020 Jan 28. Addiction. 2020. PMID: 31994226 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
