

Usefulness of Routine Fractional Flow Reserve for Clinical Management of Coronary Artery Disease in Patients With Diabetes
- PMID: 31913433
- PMCID: PMC6990935
- DOI: 10.1001/jamacardio.2019.5097
Usefulness of Routine Fractional Flow Reserve for Clinical Management of Coronary Artery Disease in Patients With Diabetes
Abstract
Importance: Approximately one-third of patients considered for coronary revascularization have diabetes, which is a major determinant of clinical outcomes, often influencing the choice of the revascularization strategy. The usefulness of fractional flow reserve (FFR) to guide treatment in this population is understudied and has been questioned.
Objective: To evaluate the usefulness and rate of major adverse cardiovascular events (MACE) of integrating FFR in management decisions for patients with diabetes who undergo coronary angiography.
Design, setting, and participants: This cross-sectional study used data from the PRIME-FFR study derived from the merger of the POST-IT study (Portuguese Study on the Evaluation of FFR-Guided Treatment of Coronary Disease [March 2012-November 2013]) and R3F study (French Study of FFR Integrated Multicenter Registries Implementation of FFR in Routine Practice [October 2008-June 2010]), 2 prospective multicenter registries that shared a common design. A population of all-comers for whom angiography disclosed ambiguous lesions was analyzed for rates, patterns, and outcomes associated with management reclassification, including revascularization deferral, in patients with vs without diabetes. Data analysis was performed from June to August 2018.
Main outcomes and measures: Death from any cause, myocardial infarction, or unplanned revascularization (MACE) at 1 year.
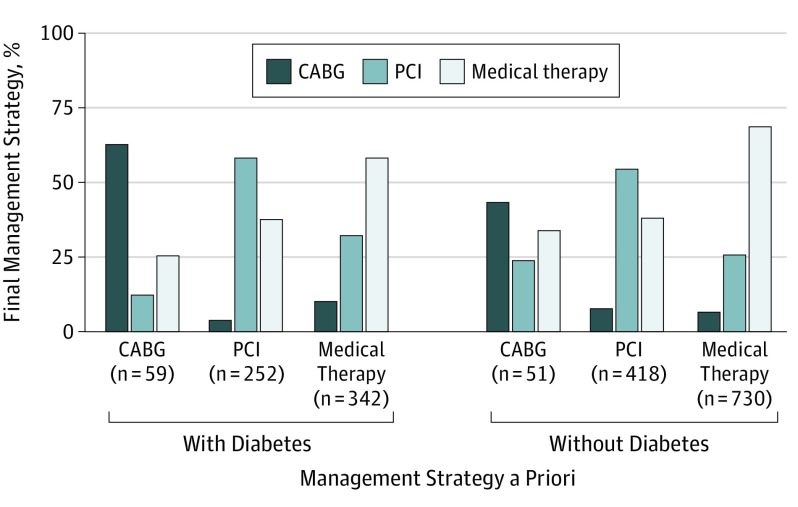
Results: Among 1983 patients (1503 [77%] male; mean [SD] age, 65 [10] years), 701 had diabetes, and FFR was performed for 1.4 lesions per patient (58.2% of lesions in the left anterior descending artery; mean [SD] stenosis, 56% [11%]; mean [SD] FFR, 0.81 [0.01]). Reclassification by FFR was high and similar in patients with and without diabetes (41.2% vs 37.5%, P = .13), but reclassification from medical treatment to revascularization was more frequent in the former (142 of 342 [41.5%] vs 230 of 730 [31.5%], P = .001). There was no statistical difference between the 1-year rates of MACE in reclassified (9.7%) and nonreclassified patients (12.0%) (P = .37). Among patients with diabetes, FFR-based deferral identified patients with a lower risk of MACE at 12 months (25 of 296 [8.4%]) compared with those undergoing revascularization (47 of 257 [13.1%]) (P = .04), and the rate was of the same magnitude of the observed rate among deferred patients without diabetes (7.9%, P = .87). Status of insulin treatment had no association with outcomes. Patients (6.6% of the population) in whom FFR was disregarded had the highest MACE rates regardless of diabetes status.
Conclusions and relevance: Routine integration of FFR for the management of coronary artery disease in patients with diabetes may be associated with a high rate of treatment reclassification. Management strategies guided by FFR, including revascularization deferral, may be useful for patients with diabetes.
Conflict of interest statement
Figures


References
-
- De Bruyne B, Pijls NH, Kalesan B, et al. ; FAME 2 Trial Investigators . Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease [published correction appears in N Engl J Med. 2012;367(18):1768]. N Engl J Med. 2012;367(11):991-1001. doi:10.1056/NEJMoa1205361 - DOI - PubMed
-
- Van Belle E, Rioufol G, Pouillot C, et al. ; Investigators of the Registre Français de la FFR–R3F . Outcome impact of coronary revascularization strategy reclassification with fractional flow reserve at time of diagnostic angiography: insights from a large French multicenter fractional flow reserve registry. Circulation. 2014;129(2):173-185. doi:10.1161/CIRCULATIONAHA.113.006646 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
