

Universal screening versus risk-based protocols for antibiotic prophylaxis during childbirth to prevent early-onset group B streptococcal disease: a systematic review and meta-analysis
- PMID: 31913562
- PMCID: PMC7187465
- DOI: 10.1111/1471-0528.16085
Universal screening versus risk-based protocols for antibiotic prophylaxis during childbirth to prevent early-onset group B streptococcal disease: a systematic review and meta-analysis
Abstract
Background: Early-onset group B streptococcal (EOGBS) disease (including sepsis, meningitis, and pneumonia) causes significant morbidity and mortality in newborn infants worldwide. Antibiotic prophylaxis can prevent vertical streptococcal transmission, yet no uniform criteria exist to identify eligible women for prophylaxis. Some guidelines recommend universal GBS screening to pregnant women in their third trimester (screening-based protocol), whereas others employ risk-based protocols.
Objectives: To compare the effectiveness of screening-based versus risk-based protocols in preventing EOGBS disease.
Search strategy: Key words for the database searches included GBS, Streptococcus agalactiae, pregnancy, screening, culture-based, risk-based.
Selection criteria: Studies were included if they investigated EOGBS disease incidence in newborn infants and compared screening or risk-based protocols with each other or with controls.
Data collection and analysis: Risk ratios (RR) and 95% confidence intervals (CI) were determined using Mantel-Haenszel analyses with random effects.
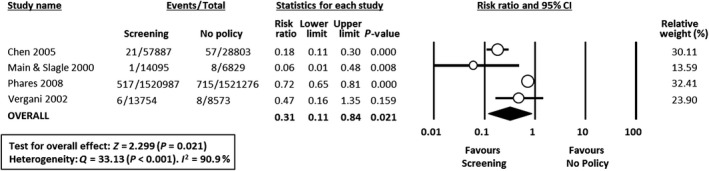
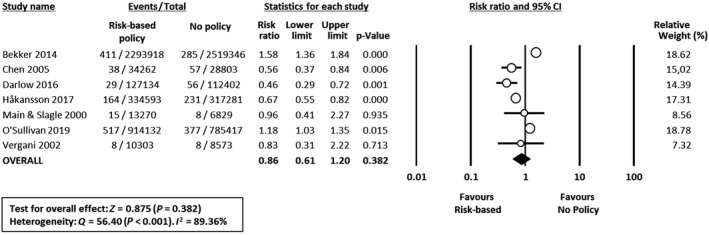
Main results: Seventeen eligible studies were included. In this meta-analysis, screening was associated with a reduced risk for EOGBS disease compared either with risk-based protocols (ten studies, RR 0.43, 95% CI 0.32-0.56) or with no policy (four studies, RR 0.31, 95% CI 0.11-0.84). Meta-analysis could not demonstrate a significant effect of risk-based protocols versus no policy (seven studies, RR 0.86, 95% CI 0.61-1.20). In studies reporting on the use of antibiotics, screening was not associated with higher antibiotic administration rates (31 versus 29%).
Conclusions: Screening-based protocols were associated with lower incidences of EOGBS disease compared with risk-based protocols, while not clearly overexposing women to antibiotics. This information is of relevance for future policymaking.
Tweetable abstract: Meta-analysis: general screening is associated with lower rates of early-onset group B strep. neonatal sepsis compared with risk-based protocols.
Keywords: Antibiotic prophylaxis; Streptococcus agalactiae; early-onset neonatal sepsis; group B streptococcus; meta-analysis; newborn infant; risk-based; screening; sepsis; streptococcal infections; systematic review; vertical transmission.
2020 The Authors. BJOG: An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd on behalf of Royal College of Obstetricians and Gynaecologists.
Figures

Comment in
-
An obstetrician's dilemma - a parody.BJOG. 2020 May;127(6):692. doi: 10.1111/1471-0528.16097. Epub 2020 Feb 9. BJOG. 2020. PMID: 31972875 No abstract available.
-
Universal testing for group B streptococcus during pregnancy: need for a randomised trial.BJOG. 2020 May;127(6):693. doi: 10.1111/1471-0528.16116. Epub 2020 Feb 27. BJOG. 2020. PMID: 31999886 No abstract available.
-
Re: Universal screening versus risk-based protocols for antibiotic prophylaxis during childbirth to prevent early-onset group B streptococcal disease: a systematic review and meta-analysis.BJOG. 2020 Jul;127(8):1038-1039. doi: 10.1111/1471-0528.16253. Epub 2020 May 10. BJOG. 2020. PMID: 32388903 No abstract available.
-
Re: Universal screening versus risk-based protocols for antibiotic prophylaxis during childbirth to prevent early-onset group B streptococcal disease: a systematic review and meta-analysis.BJOG. 2020 Aug;127(9):1167-1168. doi: 10.1111/1471-0528.16298. Epub 2020 May 22. BJOG. 2020. PMID: 32441455 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
