

Burden and Timeline of Infectious Diseases in the First Year After Solid Organ Transplantation in the Swiss Transplant Cohort Study
- PMID: 31915816
- PMCID: PMC7583409
- DOI: 10.1093/cid/ciz1113
Burden and Timeline of Infectious Diseases in the First Year After Solid Organ Transplantation in the Swiss Transplant Cohort Study
Abstract
Background: The burden and timeline of posttransplant infections are not comprehensively documented in the current era of immunosuppression and prophylaxis.
Methods: In this prospective study nested within the Swiss Transplant Cohort Study (STCS), all clinically relevant infections were identified by transplant-infectious diseases physicians in persons receiving solid organ transplant (SOT) between May 2008 and December 2014 with ≥12 months of follow-up.
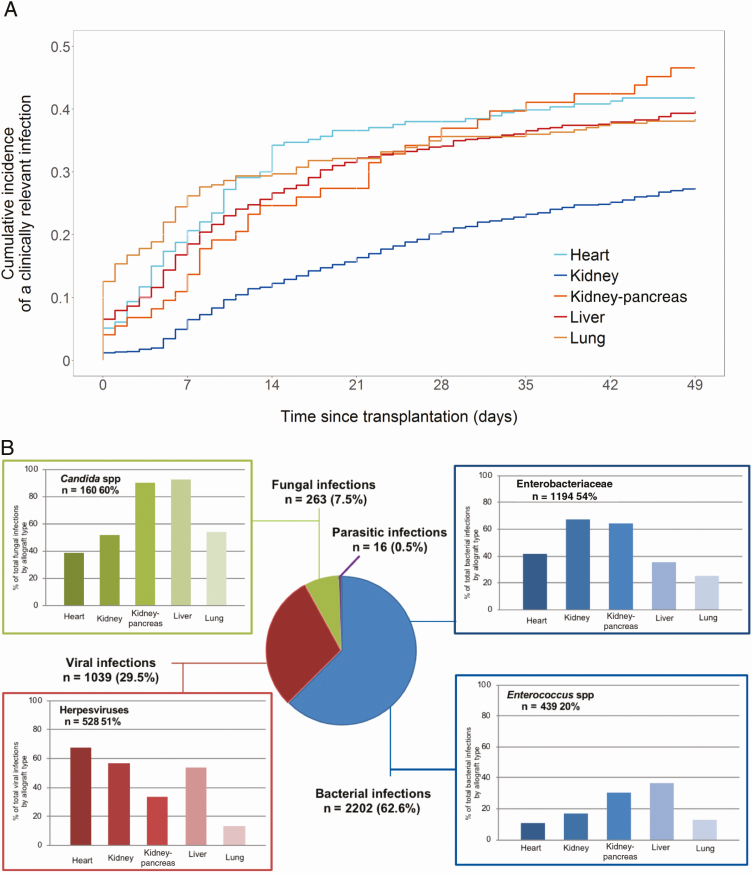
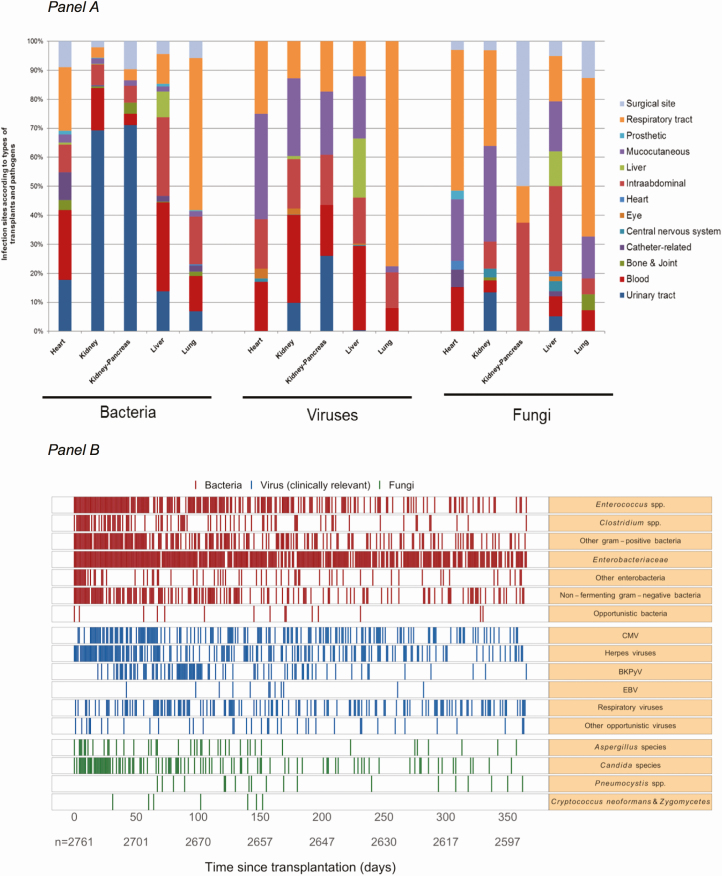
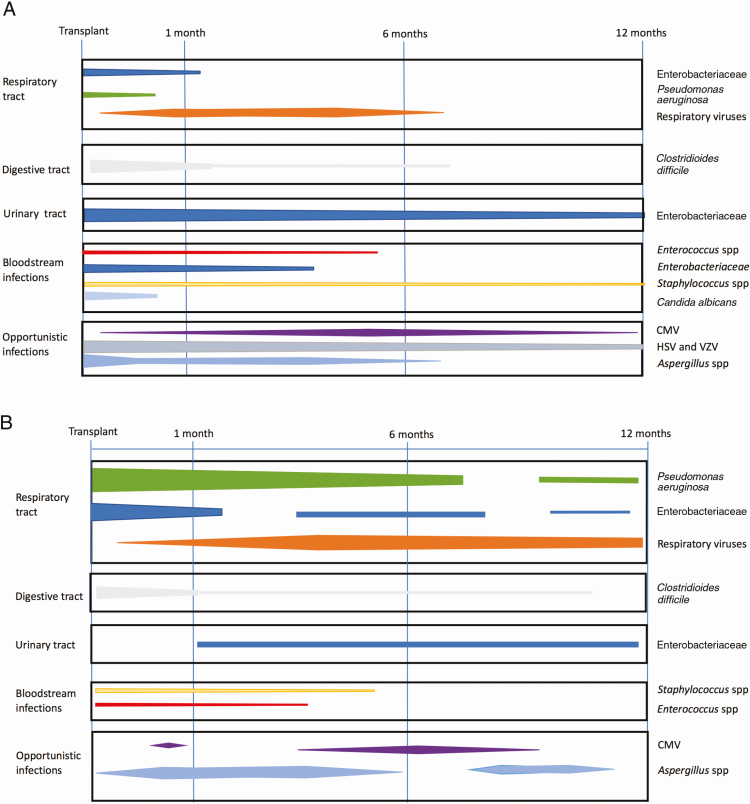
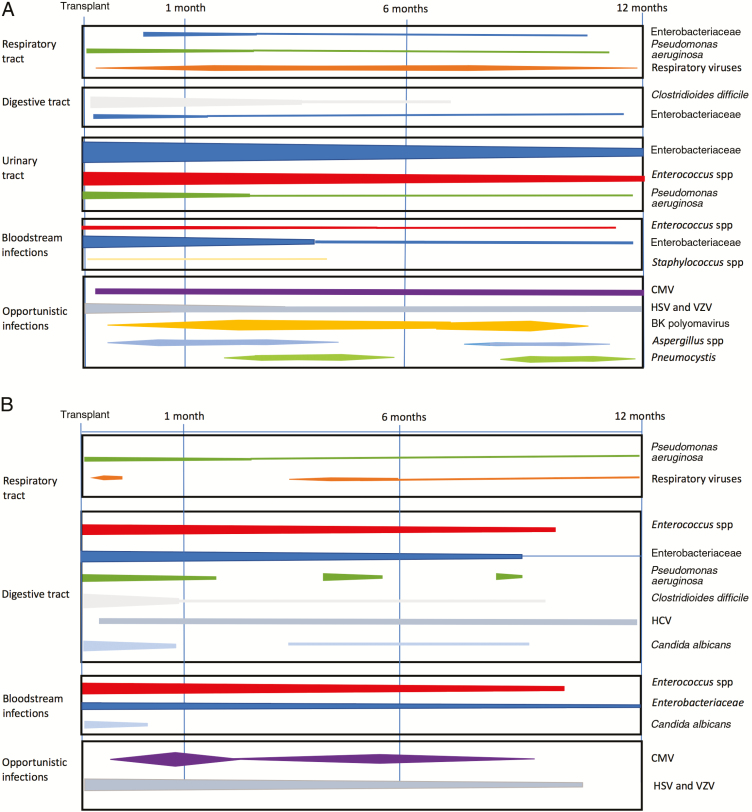
Results: Among 3541 SOT recipients, 2761 (1612 kidney, 577 liver, 286 lung, 213 heart, and 73 kidney-pancreas) had ≥12 months of follow-up; 1520 patients (55%) suffered 3520 infections during the first year posttransplantation. Burden and timelines of clinically relevant infections differed between transplantations. Bacteria were responsible for 2202 infections (63%) prevailing throughout the year, with a predominance of Enterobacteriaceae (54%) as urinary pathogens in heart, lung, and kidney transplant recipients, and as digestive tract pathogens in liver transplant recipients. Enterococcus spp (20%) occurred as urinary tract pathogens in kidney transplant recipients and as digestive tract pathogens in liver transplant recipients, and Pseudomonas aeruginosa (9%) in lung transplant recipients. Among 1039 viral infections, herpesviruses predominated (51%) in kidney, liver, and heart transplant recipients. Among 263 fungal infections, Candida spp (60%) prevailed as digestive tract pathogens in liver transplant recipients. Opportunistic pathogens, including Aspergillus fumigatus (1.4%) and cytomegalovirus (6%), were rare, scattering over 12 months across all SOT recipients.
Conclusions: In the current era of immunosuppression and prophylaxis, SOT recipients experience a high burden of infections throughout the first year posttransplantation, with rare opportunistic pathogens and a predominance of bacteria.
Keywords: bacterial; fungal; infection; solid organ transplant; viral.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Reply to Sultan et al.Clin Infect Dis. 2021 Jan 23;72(1):179. doi: 10.1093/cid/ciaa431. Clin Infect Dis. 2021. PMID: 32282037 No abstract available.
-
The Global Emergence of the Fungal Pathogen Candida auris.Clin Infect Dis. 2021 Jan 23;72(1):178-179. doi: 10.1093/cid/ciaa572. Clin Infect Dis. 2021. PMID: 32421181 No abstract available.
References
-
- Fishman JA, Rubin RH. Infection in organ-transplant recipients. N Engl J Med 1998; 338:1741–51. - PubMed
-
- Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med 2007; 357:2601–14. - PubMed
-
- Fishman JA. Infection in organ transplantation. Am J Transplant 2017; 17:856–79. - PubMed
-
- Garrido RS, Aguado JM, Díaz-Pedroche C, et al. A review of critical periods for opportunistic infection in the new transplantation era. Transplantation 2006; 82:1457–62. - PubMed
-
- San Juan R, Aguado JM, Lumbreras C, et al. RESITRA Network Incidence, clinical characteristics and risk factors of late infection in solid organ transplant recipients: data from the RESITRA study group. Am J Transplant 2007; 7:964–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
