

Targeted Perfusion Therapy in Spinal Cord Trauma
- PMID: 31916236
- PMCID: PMC7283409
- DOI: 10.1007/s13311-019-00820-6
Targeted Perfusion Therapy in Spinal Cord Trauma
Abstract
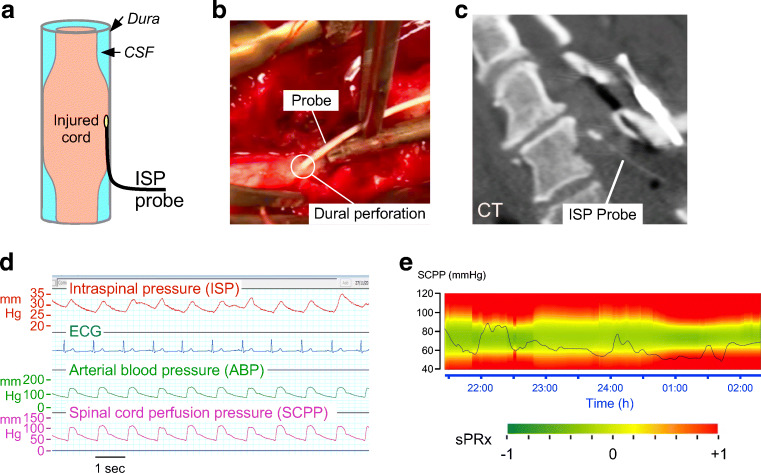
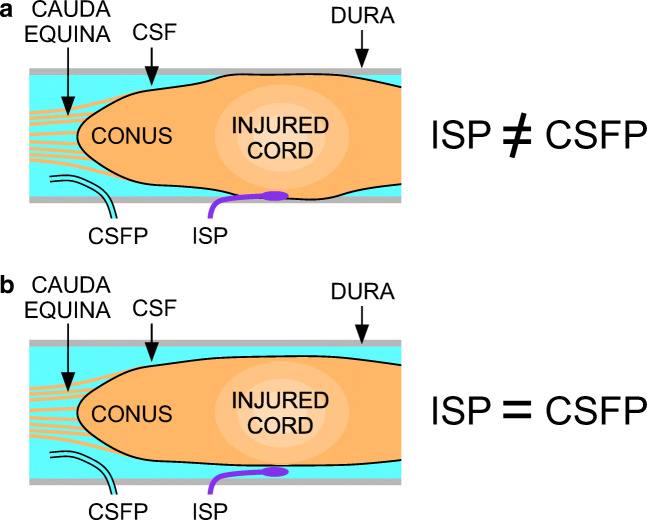
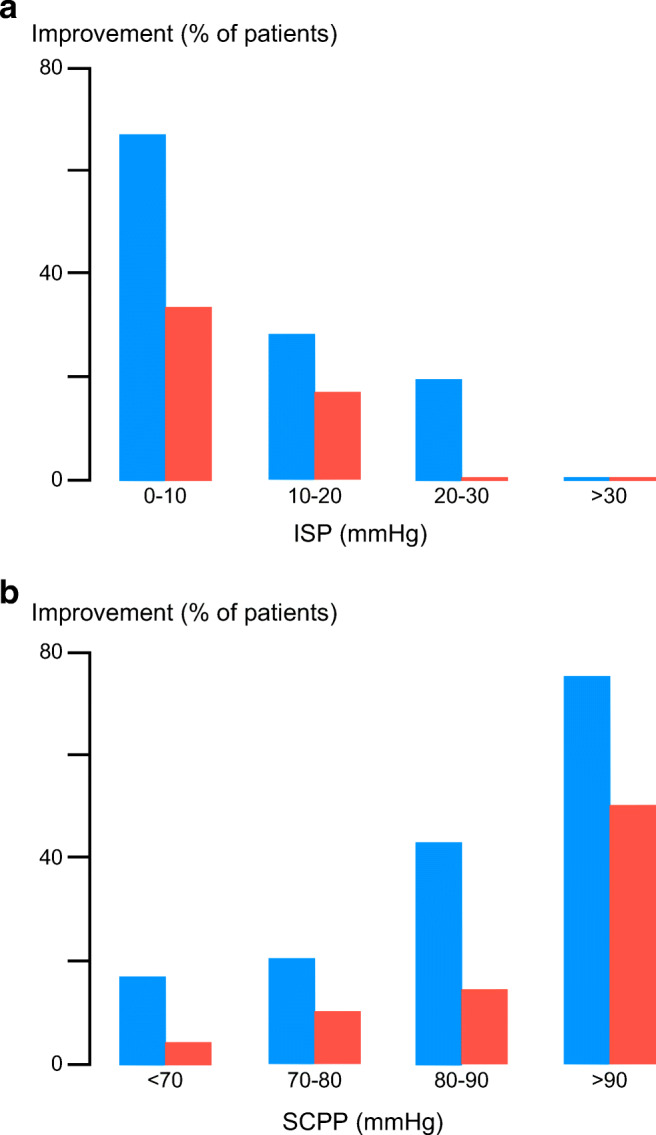
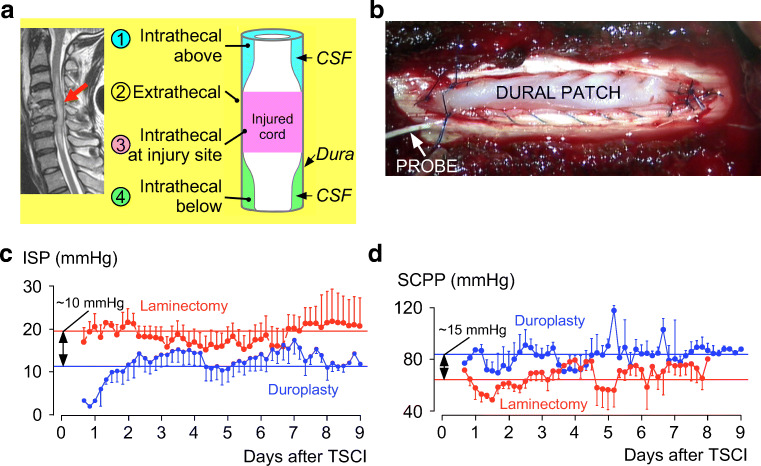
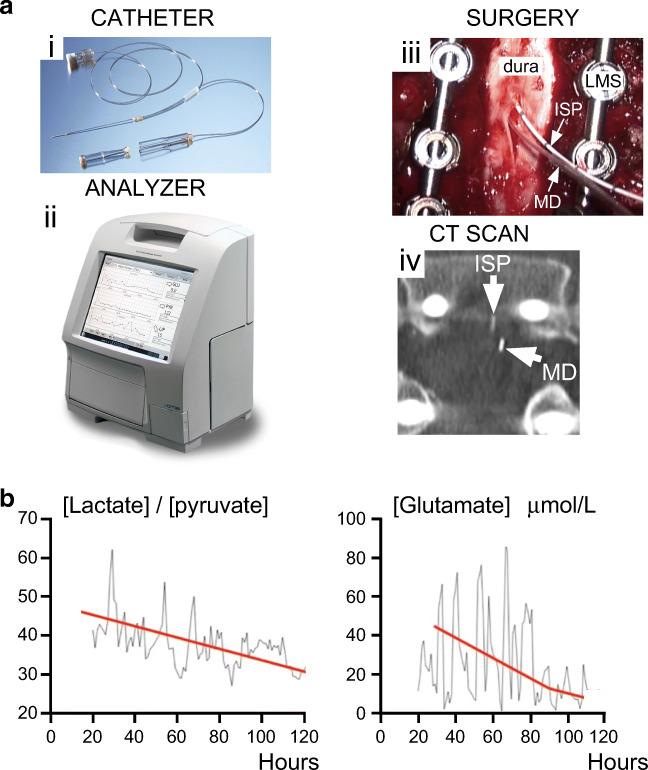
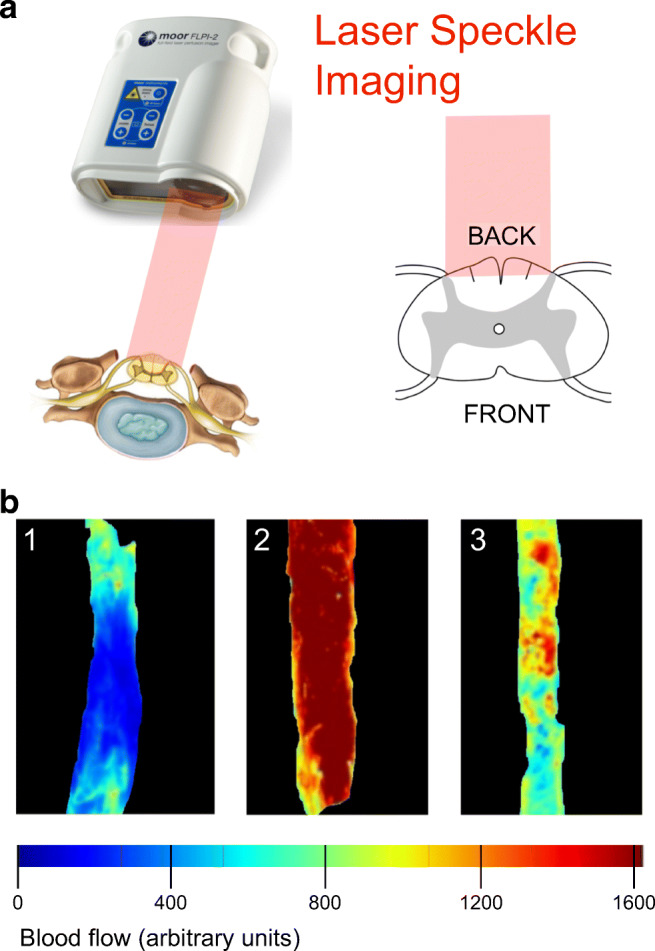
We review state-of-the-art monitoring techniques for acute, severe traumatic spinal cord injury (TSCI) to facilitate targeted perfusion of the injured cord rather than applying universal mean arterial pressure targets. Key concepts are discussed such as intraspinal pressure and spinal cord perfusion pressure (SCPP) at the injury site, respectively, analogous to intracranial pressure and cerebral perfusion pressure for traumatic brain injury. The concept of spinal cord autoregulation is introduced and quantified using spinal pressure reactivity index (sPRx), which is analogous to pressure reactivity index for traumatic brain injury. The U-shaped relationship between sPRx and SCPP defines the optimum SCPP as the SCPP that minimizes sPRx (i.e., maximizes autoregulation), and suggests that not only ischemia but also hyperemia at the injury site may be detrimental. The observation that optimum SCPP varies between patients and temporally in each patient supports individualized management. We discuss multimodality monitoring, which revealed strong correlations between SCPP and injury site metabolism (tissue glucose, lactate, pyruvate, glutamate, glycerol), monitored by surface microdialysis. Evidence is presented that the dura is a major, but unappreciated, cause of spinal cord compression after TSCI; we thus propose expansion duroplasty as a novel treatment. Monitoring spinal cord blood flow at the injury site has revealed novel phenomena, e.g., 3 distinct blood flow patterns, local steal, and diastolic ischemia. We conclude that monitoring from the injured spinal cord in the intensive care unit is a safe technique that appears to enable optimized and individualized spinal cord perfusion.
Keywords: Blood pressure; critical care; decompression; dura; monitoring; spinal cord injury.
Figures
References
-
- Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord. 2014;52:110–116. - PubMed
-
- SCI. info pages: https://www.sci-info-pages.com/facts.html 2010-15; Accessed 2019.
-
- Werndle MC, Zoumprouli A, Sedgwick P, Papadopoulos MC. Variability in the treatment of acute spinal cord injury in the United Kingdom: results of a national survey. J Neurotrauma. 2012;29:880–888. - PubMed
-
- Aarabi B, Akhtar-Danesh N, Chryssikos T et al. Efficacy of Ultra-Early (< 12 h), Early (12-24 h), and Late (>24-138.5 h) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades A, B, and C Cervical Spinal Cord Injury. J Neurotrauma 2019:In press. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
