

Associations between prescribed benzodiazepines, overdose death and buprenorphine discontinuation among people receiving buprenorphine
- PMID: 31916306
- PMCID: PMC7156323
- DOI: 10.1111/add.14886
Associations between prescribed benzodiazepines, overdose death and buprenorphine discontinuation among people receiving buprenorphine
Abstract
Background and aims: Benzodiazepines are commonly prescribed to patients with opioid use disorder receiving buprenorphine treatment, yet may increase overdose risk. However, prescribed benzodiazepines may improve retention in care by reducing buprenorphine discontinuation and thus may prevent relapse to illicit opioid use. We aimed to test the association between benzodiazepine prescription and fatal opioid overdose, non-fatal opioid overdose, all-cause mortality and buprenorphine discontinuation.
Design and setting: This was a retrospective cohort study using five individually linked data sets from Massachusetts, United States government agencies.
Participants: We studied 63 389 Massachusetts residents aged 18 years or older who received buprenorphine treatment between January 2012 and December 2015.
Measurements: Filled benzodiazepine prescription during buprenorphine treatment was the main independent variable. The primary outcome was time to fatal opioid overdose. Secondary outcomes were time to non-fatal opioid overdose, all-cause mortality and buprenorphine discontinuation. We defined buprenorphine discontinuation as having a 30-day gap without another prescription following the end date of the previous prescription. We used Cox proportional hazards models to calculate hazards ratios that tested the association between receipt of benzodiazepines and all outcomes, restricted to periods during buprenorphine treatment.
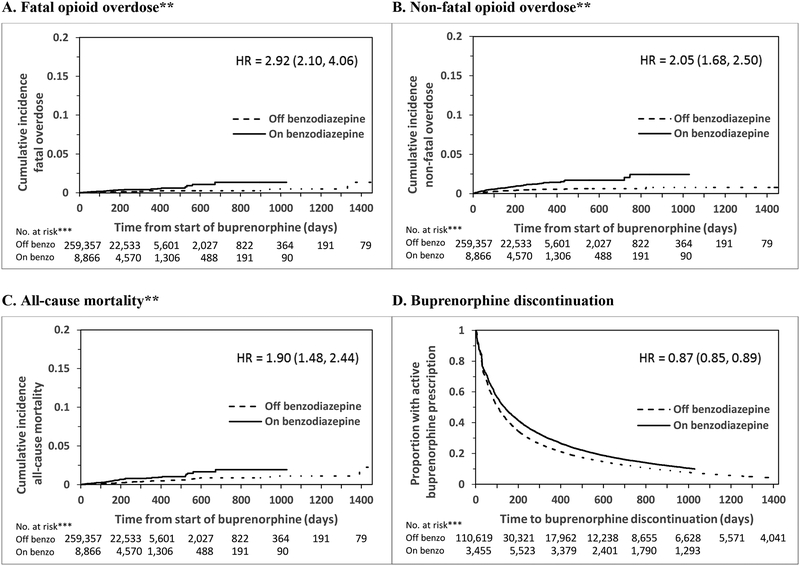
Findings: Of the 63 345 individuals who received buprenorphine, 24% filled at least one benzodiazepine prescription during buprenorphine treatment. Thirty-one per cent of the 183 deaths from opioid overdose occurred when individuals received benzodiazepines during buprenorphine treatment. Benzodiazepine receipt during buprenorphine treatment was associated with an increased risk of fatal opioid overdose adjusted hazard ratio (HR) = 2.92, 95% confidence interval (CI) = 2.10-4.06, non-fatal opioid overdose, adjusted HR = 2.05, 95% CI, 1.68-2.50, all-cause mortality, adjusted HR = 1.90, 95% CI, 1.48-2.44 and a decreased risk of buprenorphine discontinuation, adjusted HR = 0.87, 95% CI, 0.85-0.89.
Conclusions: Benzodiazepine receipt appears to be associated with both increased risk of opioid overdose and all-cause mortality and decreased risk of buprenorphine discontinuation among people receiving buprenorphine.
Keywords: benzodiazepines; buprenorphine; buprenorphine discontinuation; cohort study; opioids; overdose.
© 2020 Society for the Study of Addiction.
Figures
Comment in
-
Commentary on Park et al. (2020): Buprenorphine and benzodiazepine co-prescribing- key considerations and future directions.Addiction. 2020 May;115(5):933-934. doi: 10.1111/add.14990. Epub 2020 Feb 20. Addiction. 2020. PMID: 32077171 No abstract available.
Similar articles
-
Medication for Opioid Use Disorder After Nonfatal Opioid Overdose and Association With Mortality: A Cohort Study.Ann Intern Med. 2018 Aug 7;169(3):137-145. doi: 10.7326/M17-3107. Epub 2018 Jun 19. Ann Intern Med. 2018. PMID: 29913516 Free PMC article.
-
Patient outcomes following buprenorphine treatment for opioid use disorder: A retrospective analysis of the influence of patient- and prescriber-level characteristics in Massachusetts, USA.Addiction. 2025 Jan;120(1):152-163. doi: 10.1111/add.16684. Epub 2024 Oct 13. Addiction. 2025. PMID: 39397274 Free PMC article.
-
Opioid agonist treatment and fatal overdose risk in a state-wide US population receiving opioid use disorder services.Addiction. 2020 Sep;115(9):1683-1694. doi: 10.1111/add.14991. Epub 2020 Feb 24. Addiction. 2020. PMID: 32096302 Free PMC article.
-
Effects of medication-assisted treatment on mortality among opioids users: a systematic review and meta-analysis.Mol Psychiatry. 2019 Dec;24(12):1868-1883. doi: 10.1038/s41380-018-0094-5. Epub 2018 Jun 22. Mol Psychiatry. 2019. PMID: 29934549
-
The association between benzodiazepine co-prescription, opioid agonist treatment and mortality: a systematic review.BMC Psychiatry. 2024 Oct 28;24(1):741. doi: 10.1186/s12888-024-06191-3. BMC Psychiatry. 2024. PMID: 39468492 Free PMC article.
Cited by
-
Identifying and Treating Incarcerated Women Experiencing Substance Use Disorders: A Review.Subst Abuse Rehabil. 2023 Nov 13;14:131-145. doi: 10.2147/SAR.S409944. eCollection 2023. Subst Abuse Rehabil. 2023. PMID: 38026785 Free PMC article. Review.
-
Polysubstance use before and during treatment with medication for opioid use disorder: Prevalence and association with treatment outcomes.J Subst Abuse Treat. 2022 Dec;143:108830. doi: 10.1016/j.jsat.2022.108830. Epub 2022 Jun 22. J Subst Abuse Treat. 2022. PMID: 35773113 Free PMC article. Clinical Trial.
-
Fatalities in opioid agonist treatment with long-acting injectable buprenorphine.Int J Legal Med. 2025 Jun 18. doi: 10.1007/s00414-025-03535-w. Online ahead of print. Int J Legal Med. 2025. PMID: 40531311
-
Benzodiazepine agonist treatment for patients with benzodiazepine dependence undergoing opioid agonist treatment: a study protocol for the randomized controlled trial BMX-BAR.Trials. 2025 Jan 2;26(1):2. doi: 10.1186/s13063-024-08692-8. Trials. 2025. PMID: 39748420 Free PMC article.
-
The Opioid-overdose Reduction Continuum of Care Approach (ORCCA): Evidence-based practices in the HEALing Communities Study.Drug Alcohol Depend. 2020 Dec 1;217:108325. doi: 10.1016/j.drugalcdep.2020.108325. Epub 2020 Oct 4. Drug Alcohol Depend. 2020. PMID: 33091842 Free PMC article.
References
-
- Piper BJ, Shah DT, Simoyan OM, McCall KL, Nichols SD. Trends in Medical Use of Opioids in the U.S., 2006–2016. American Journal of Preventive Medicine. 2018. May 1;54(5):652–60. - PubMed
-
- Gueye PN, Borron SW, Risède P, Monier C, Buneaux F, Debray M, et al. Buprenorphine and midazolam act in combination to depress respiration in rats. Toxicol Sci. 2002. January;65(1):107–14. - PubMed
-
- Borron SW, Monier C, Risède P, Baud FJ. Flunitrazepam variably alters morphine, buprenorphine, and methadone lethality in the rat. Hum Exp Toxicol. 2002. November;21(11):599–605. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
