

Nutrition interventions to treat low muscle mass in cancer
- PMID: 31916411
- PMCID: PMC7113510
- DOI: 10.1002/jcsm.12525
Nutrition interventions to treat low muscle mass in cancer
Abstract
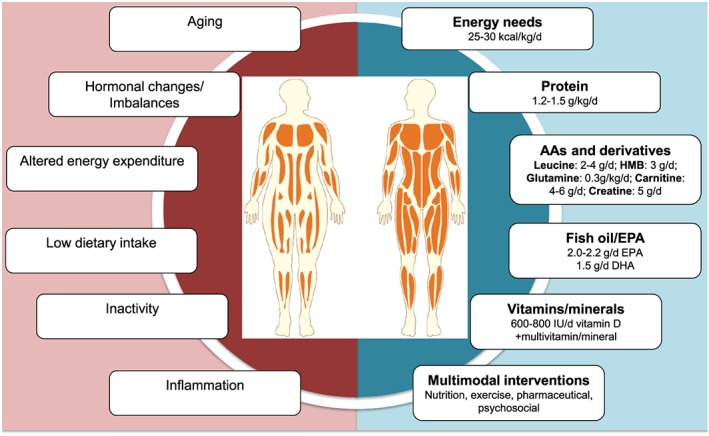
Many patients with cancer experience poor nutritional status, which detrimentally impacts clinical outcomes. Poor nutritional status in cancer is primarily manifested by severe muscle mass (MM) depletion, which may occur at any stage (from curative to palliative) and often co-exists with obesity. The objective of this article was to discuss gaps and opportunities related to the role of nutrition in preventing and reversing low MM in cancer. It also provides a narrative review of relevant nutritional interventions for patients capable of oral intake. The impact of nutrition interventions to prevent/treat low MM in cancer is not well understood, potentially due to the limited number of studies and of clinically viable, accurate body composition assessment tools. Additionally, the type of study designs, inclusion criteria, length of intervention, and choice of nutritional strategies have not been optimal, likely underestimating the anabolic potential of nutrition interventions. Nutrition studies are also often of short duration, and interventions that adapt to the metabolic and behavioural changes during the clinical journey are needed. We discuss energy requirements (25-30 kcal/kg/day) and interventions of protein (1.0-1.5 g/kg/day), branched-chain amino acids (leucine: 2-4 g/day), β-hydroxy β-methylbutyrate (3 g/day), glutamine (0.3 g/kg/day), carnitine (4-6 g/day), creatine (5 g/day), fish oil/eicosapentanoic acid (2.0-2.2 g/day EPA and 1.5 g/day DHA), vitamin/minerals (e.g. vitamin D: 600-800 international units per day), and multimodal approaches (nutrition, exercise, and pharmaceutical) to countermeasure low MM in cancer. Although the evidence is variable by modality type, interventions were generally not specifically studied in the context of cancer. Understanding patients' nutritional requirements could lead to targeted prescriptions to prevent or attenuate low MM in cancer, with the overall aim of minimizing muscle loss during anti-cancer therapy and maximizing muscle anabolism during recovery. It is anticipated that this will, in turn, improve overall health and prognostication including tolerance to treatment and survival. However, oncology-specific interventions with more robust study designs are needed to facilitate these goals.
Keywords: Body composition; Cancer; Intervention; Low muscle mass; Myopenia; Nutrition; Protein; Sarcopenia.
© 2020 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Ravasco P, Monteiro‐Grillo I, Camilo ME. Does nutrition influence quality of life in cancer patients undergoing radiotherapy? Radiother Oncol 2003;67:213–220. - PubMed
-
- Prado CMM. Body composition in chemotherapy: the promising role of CT scans. Curr Opin Clin Nutr Metab Care 2013;16:525–533. - PubMed
-
- Prado CMM, Lieffers JR, McCargar LJ, Reiman T, Sawyer MB, Martin L, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population‐based study. Lancet Oncol 2008;9:629–635. - PubMed
-
- Prado CMM, Lieffers JR, Bowthorpe L, Baracos VE, Mourtzakis M, McCargar LJ. Sarcopenia and physical function in overweight patients with advanced cancer. Can J Diet Pract Res 2013;74:69–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
