

Genetic Admixture and Survival in Diverse Populations with Pulmonary Arterial Hypertension
- PMID: 31916850
- PMCID: PMC7258627
- DOI: 10.1164/rccm.201907-1447OC
Genetic Admixture and Survival in Diverse Populations with Pulmonary Arterial Hypertension
Abstract
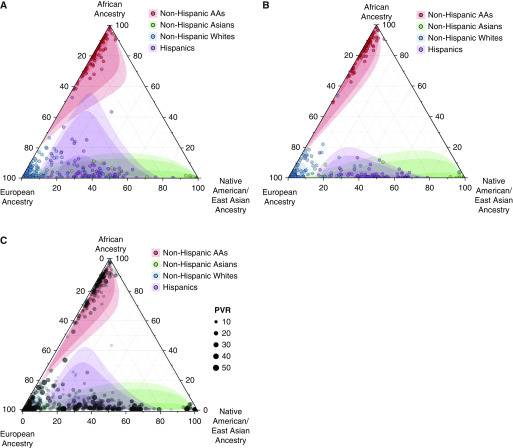
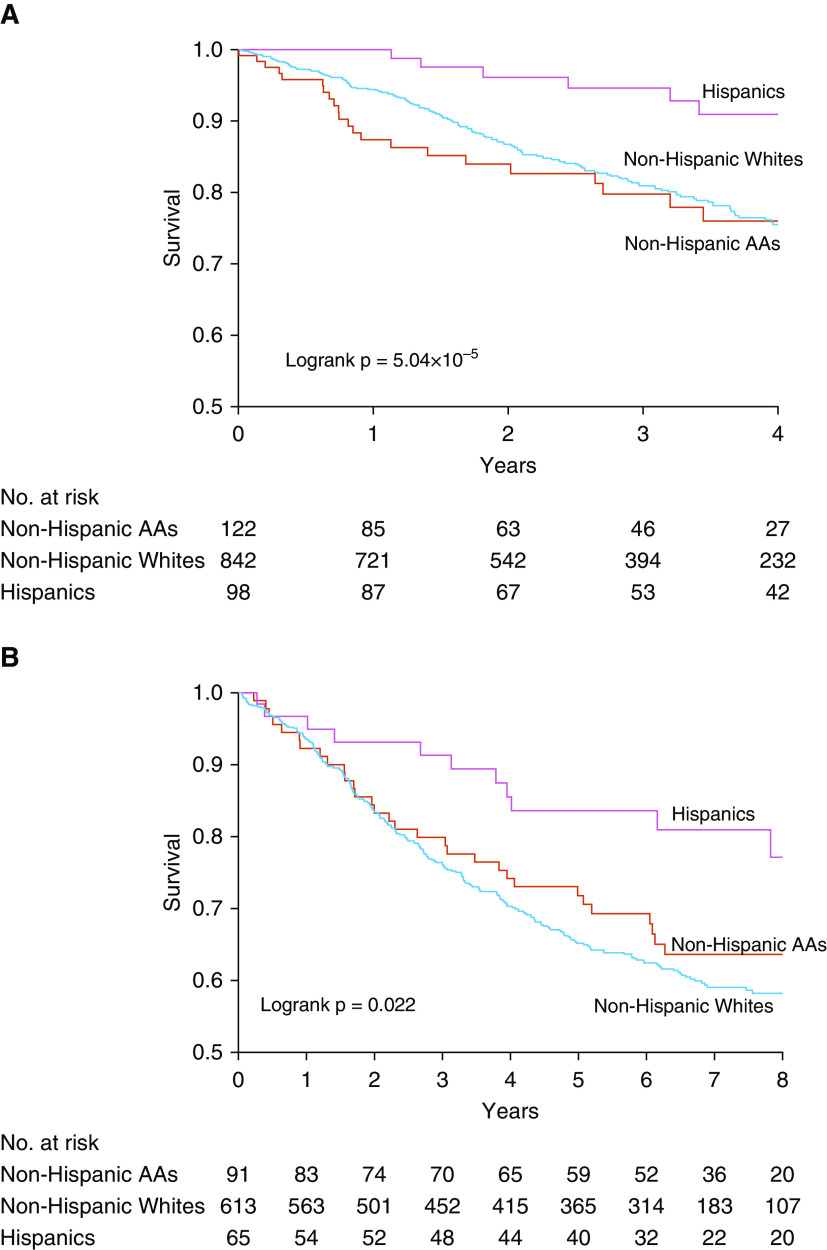
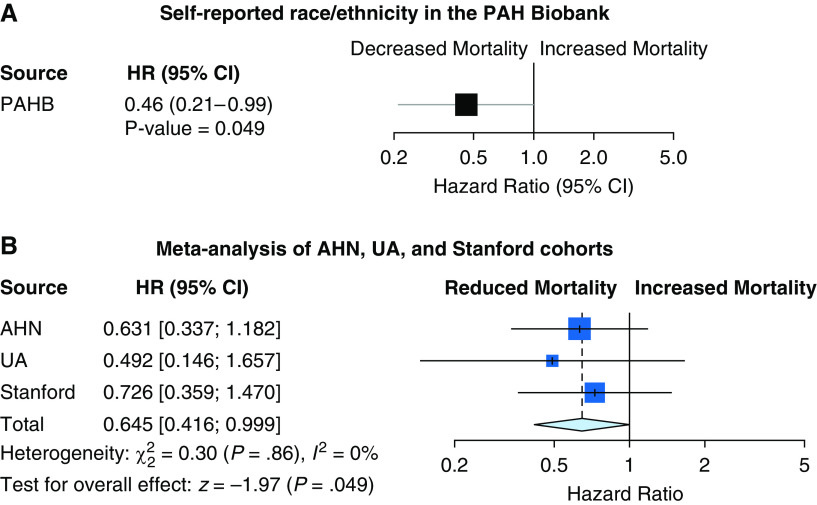
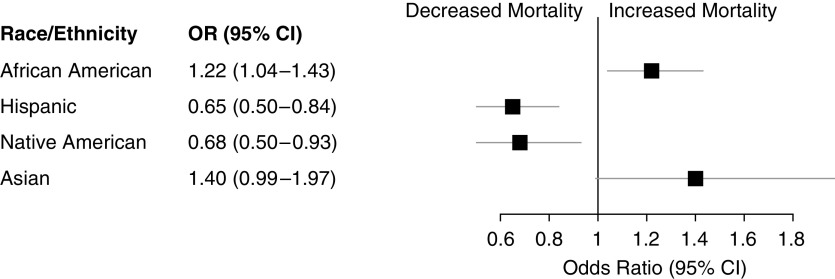
Rationale: Limited information is available on racial/ethnic differences in pulmonary arterial hypertension (PAH).Objectives: Determine effects of race/ethnicity and ancestry on mortality and disease outcomes in diverse patients with PAH.Methods: Patients with Group 1 PAH were included from two national registries with genome-wide data and two local cohorts, and further incorporated in a global meta-analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated for transplant-free, all-cause mortality in Hispanic patients with non-Hispanic white (NHW) patients as the reference group. Odds ratios (ORs) for inpatient-specific mortality in patients with PAH were also calculated for race/ethnic groups from an additional National Inpatient Sample dataset not included in the meta-analysis.Measurements and Main Results: After covariate adjustment, self-reported Hispanic patients (n = 290) exhibited significantly reduced mortality versus NHW patients (n = 1,970) after global meta-analysis (HR, 0.60 [95% CI, 0.41-0.87]; P = 0.008). Although not significant, increasing Native American genetic ancestry appeared to account for part of the observed mortality benefit (HR, 0.48 [95% CI, 0.23-1.01]; P = 0.053) in the two national registries. Finally, in the National Inpatient Sample, an inpatient mortality benefit was also observed for Hispanic patients (n = 1,524) versus NHW patients (n = 8,829; OR, 0.65 [95% CI, 0.50-0.84]; P = 0.001). An inpatient mortality benefit was observed for Native American patients (n = 185; OR, 0.38 [95% CI, 0.15-0.93]; P = 0.034).Conclusions: This study demonstrates a reproducible survival benefit for Hispanic patients with Group 1 PAH in multiple clinical settings. Our results implicate contributions of genetic ancestry to differential survival in PAH.
Keywords: Hispanic American; Native American; health disparities; pulmonary arterial hypertension; survival.
Figures
Comment in
-
Deconstructing the Melting Pot in Pulmonary Arterial Hypertension.Am J Respir Crit Care Med. 2020 Jun 1;201(11):1329-1331. doi: 10.1164/rccm.202001-0156ED. Am J Respir Crit Care Med. 2020. PMID: 32053755 Free PMC article. No abstract available.
-
Challenging the Role of Genetic Ancestry in Explaining Racial/Ethnic Health Disparities.Am J Respir Crit Care Med. 2021 Feb 1;203(3):397-398. doi: 10.1164/rccm.202009-3636LE. Am J Respir Crit Care Med. 2021. PMID: 33125255 Free PMC article. No abstract available.
-
Reply to Non and Chang: Challenging the Role of Genetic Ancestry in Explaining Racial/Ethnic Health Disparities.Am J Respir Crit Care Med. 2021 Feb 1;203(3):398-399. doi: 10.1164/rccm.202010-3846LE. Am J Respir Crit Care Med. 2021. PMID: 33125257 Free PMC article. No abstract available.
References
-
- Runo JR, Loyd JE. Primary pulmonary hypertension. Lancet. 2003;361:1533–1544. - PubMed
-
- Lau EMT, Giannoulatou E, Celermajer DS, Humbert M. Epidemiology and treatment of pulmonary arterial hypertension. Nat Rev Cardiol. 2017;14:603–614. - PubMed
-
- Farber HW, Miller DP, Poms AD, Badesch DB, Frost AE, Muros-Le Rouzic E, et al. Five-year outcomes of patients enrolled in the REVEAL Registry. Chest. 2015;148:1043–1054. - PubMed
