

Pitolisant for Daytime Sleepiness in Patients with Obstructive Sleep Apnea Who Refuse Continuous Positive Airway Pressure Treatment. A Randomized Trial
- PMID: 31917607
- PMCID: PMC7193861
- DOI: 10.1164/rccm.201907-1284OC
Pitolisant for Daytime Sleepiness in Patients with Obstructive Sleep Apnea Who Refuse Continuous Positive Airway Pressure Treatment. A Randomized Trial
Erratum in
-
Erratum: Pitolisant for Daytime Sleepiness in Patients with Obstructive Sleep Apnea Who Refuse Continuous Positive Airway Pressure Treatment. A Randomized Trial.Am J Respir Crit Care Med. 2020 Jul 1;202(1):154-155. doi: 10.1164/rccm.v202erratum1. Am J Respir Crit Care Med. 2020. PMID: 32609018 Free PMC article. No abstract available.
Abstract
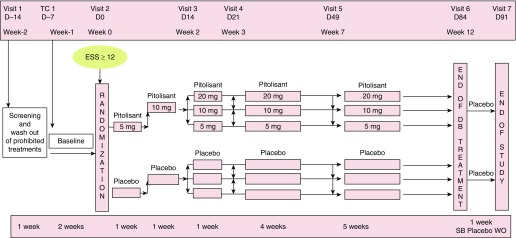
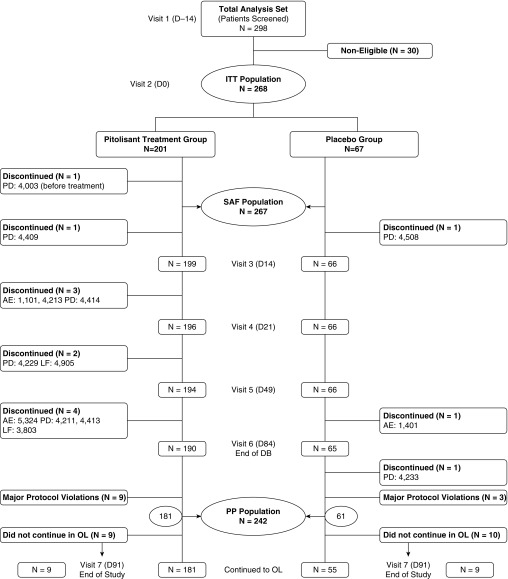
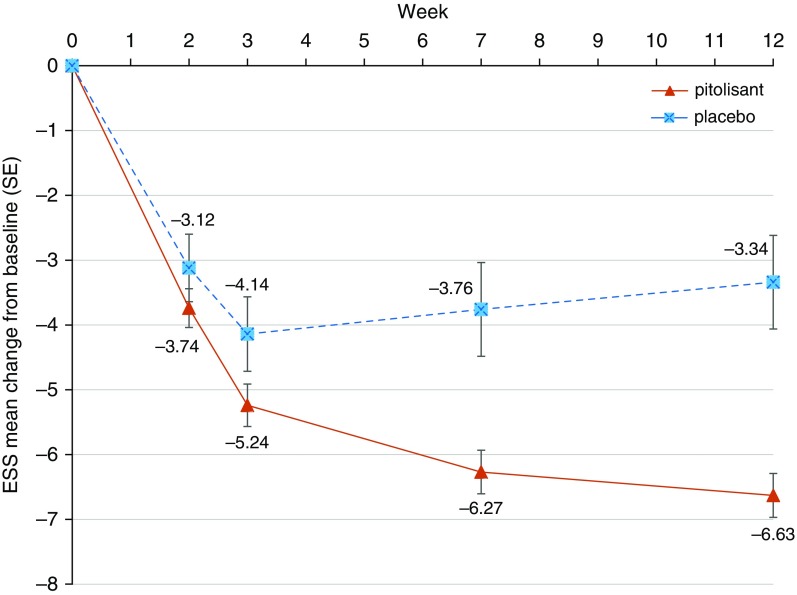
Rationale: Excessive daytime sleepiness is a common disabling symptom in obstructive sleep apnea syndrome.Objectives: To evaluate the efficacy and safety of pitolisant, a selective histamine H3 receptor antagonist with wake-promoting effects, for the treatment of daytime sleepiness in patients with moderate to severe obstructive sleep apnea refusing continuous positive airway pressure treatment.Methods: In an international, multicenter, double-blind, randomized (3:1), placebo-controlled, parallel-design trial, pitolisant was individually titrated at up to 20 mg/d over 12 weeks. The primary endpoint was the change in the Epworth Sleepiness Scale score. Key secondary endpoints were maintenance of wakefulness assessed on the basis of the Oxford Sleep Resistance test, safety, Clinical Global Impression of severity, patient's global opinion, EuroQol quality-of-life questionnaire, and Pichot fatigue questionnaire.Measurements and Main Results: A total of 268 patients with obstructive sleep apnea (75% male; mean age, 52 yr; apnea-hypopnea index, 49/h; baseline sleepiness score, 15.7) were randomized (200 to pitolisant and 68 to placebo) and analyzed on an intention-to-treat basis. The Epworth Sleepiness Scale score was reduced more with pitolisant than with placebo (-2.8; 95% confidence interval, -4.0 to -1.5; P < 0.001). Wake maintenance tests were not improved. The Pichot fatigue score was reduced with pitolisant. The overall impact of pitolisant was confirmed by both physicians' and patients' questionnaires. Adverse event incidence, mainly headache, insomnia, nausea, and vertigo, was similar in the pitolisant and placebo groups (29.5% and 25.4%, respectively), with no cardiovascular or other significant safety concerns.Conclusions: Pitolisant significantly reduced self-reported daytime sleepiness and fatigue and improved patient-reported outcomes and physician disease severity assessment in sleepy patients with obstructive sleep apnea refusing or nonadherent to continuous positive airway pressure.Clinical trial registered with www.clinicaltrials.gov (NCT01072968) and EU Clinical Trials Register (EudraCT 2009-017251-94).
Keywords: continuous positive airway pressure; excessive daytime sleepiness; obstructive sleep apnea; pitolisant.
Figures
Comment in
-
Treat the Symptom, Not the Cause? Pitolisant for Sleepiness in Obstructive Sleep Apnea.Am J Respir Crit Care Med. 2020 May 1;201(9):1033-1035. doi: 10.1164/rccm.202001-0104ED. Am J Respir Crit Care Med. 2020. PMID: 31990205 Free PMC article. No abstract available.
References
-
- Lévy P, Kohler M, McNicholas WT, Barbé F, McEvoy RD, Somers VK, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers. 2015;1:15015. - PubMed
-
- McNicholas WT, Bassetti CL, Ferini-Strambi L, Pépin JL, Pevernagie D, Verbraecken J, et al. Baveno Working Group. Challenges in obstructive sleep apnoea. Lancet Respir Med. 2018;6:170–172. - PubMed
-
- Rosenzweig I, Glasser M, Polsek D, Leschziner GD, Williams SC, Morrell MJ. Sleep apnoea and the brain: a complex relationship. Lancet Respir Med. 2015;3:404–414. - PubMed
-
- Bucks RS, Olaithe M, Rosenzweig I, Morrell MJ. Reviewing the relationship between OSA and cognition: where do we go from here? Respirology. 2017;22:1253–1261. - PubMed
-
- Bratton DJ, Gaisl T, Schlatzer C, Kohler M. Comparison of the effects of continuous positive airway pressure and mandibular advancement devices on sleepiness in patients with obstructive sleep apnoea: a network meta-analysis. Lancet Respir Med. 2015;3:869–878. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
