

Adrenocortical carcinoma masquerading as pheochromocytoma: a histopathologic dilemma
- PMID: 31917677
- PMCID: PMC6993251
- DOI: 10.1530/EDM-19-0147
Adrenocortical carcinoma masquerading as pheochromocytoma: a histopathologic dilemma
Abstract
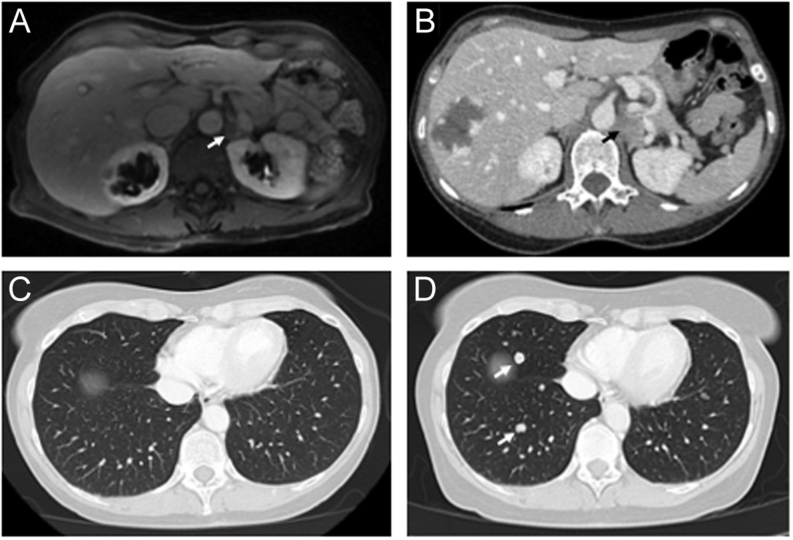
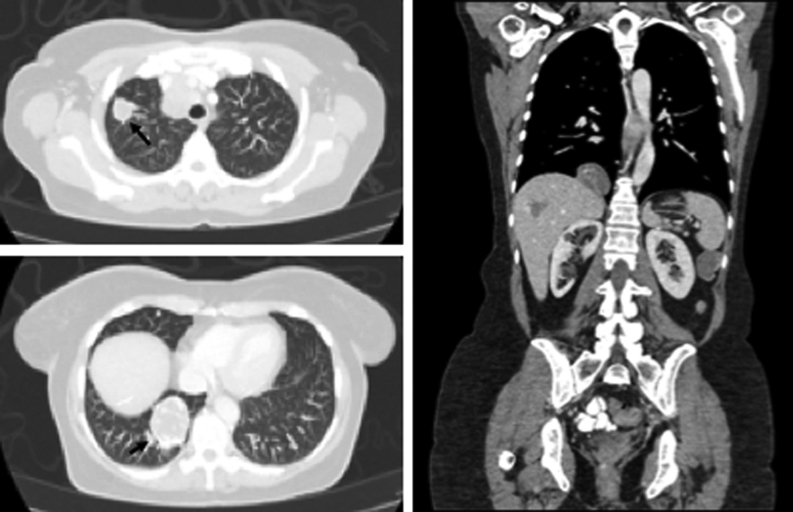
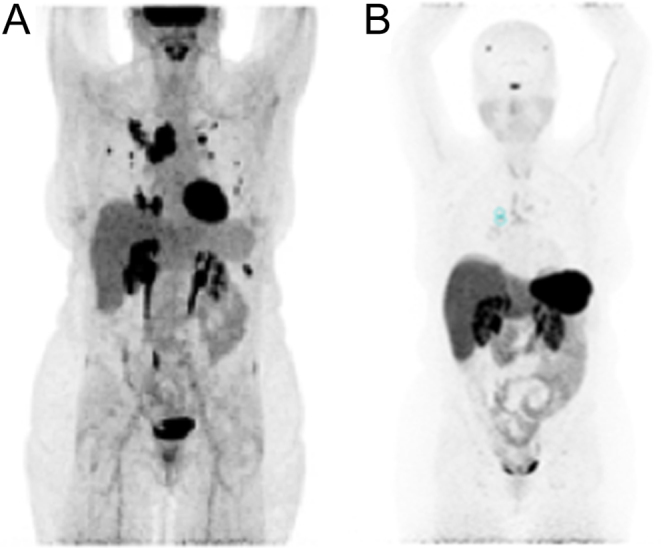
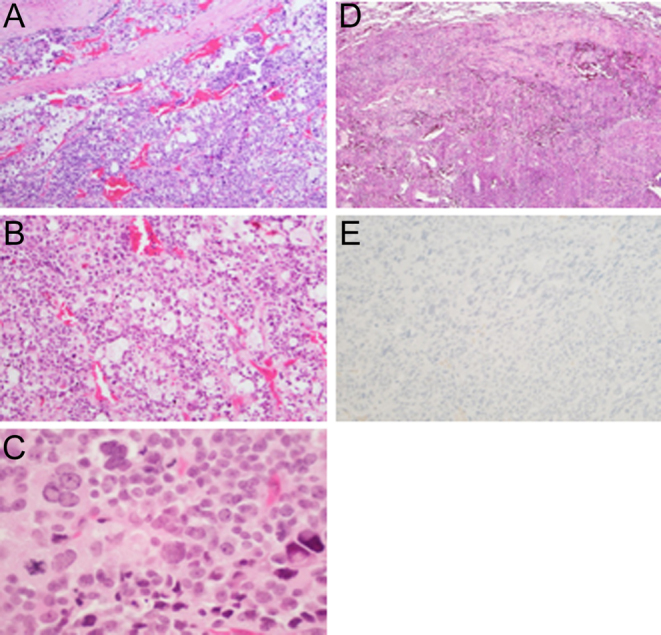
Summary: Adrenocortical carcinoma (ACC) is an aggressive cancer that originates in the cortex of the adrenal gland and generally has a poor prognosis. ACC is rare but can be more commonly seen in those with cancer predisposition syndromes (e.g. Li-Fraumeni and Lynch Syndrome). The diagnosis of ACC is sometimes uncertain and it requires the use of precise molecular pathology; the differential diagnosis includes pheochromocytoma, adrenal adenoma, renal carcinoma, or hepatocellular carcinoma. We describe a case of a 57-year-old woman with Lynch Syndrome and metastatic ACC who was initially diagnosed as having pheochromocytoma. The tumor was first identified at 51 years of age by ultrasound followed by a CT scan. She underwent a left adrenalectomy, and the histopathology identified pheochromocytoma. Two years later, she had tumor recurrence with imaging studies showing multiple lung nodules. Following a wedge resection by video-assisted thoracoscopic surgery (VATS), histopathology was read as metastatic pheochromocytoma at one institution and metastatic ACC at another institution. She later presented to the National Institutes of Health (NIH) where the diagnosis of ACC was confirmed. Following her ACC diagnosis, she was treated with mitotane and pembrolizumab which were stopped due to side effects and progression of disease. She is currently receiving etoposide, doxorubicin, and cisplatin (EDP). This case highlights the importance of using a multi-disciplinary approach in patient care. Thorough evaluation of the tumor's pathology and analysis of the patient's genetic profile are necessary to obtain the correct diagnosis for the patient and can significantly influence the course of treatment.
Learning points: Making the diagnosis of ACC can be difficult as the differential diagnosis includes pheochromocytoma, adrenal adenoma, renal carcinoma, or hepatocellular carcinoma. Patients with Lynch Syndrome should undergo surveillance for ACC as there is evidence of an association between Lynch Syndrome and ACC. Conducting a complete tumor immunoprofile and obtaining a second opinion is very important in cases of suspected ACC in order to confirm the proper diagnosis. A multi-disciplinary approach including genetic testing and a thorough evaluation of the tumor's pathology is imperative to ensuring that the patient receives an accurate diagnosis and the appropriate treatment.
Keywords: 2020; Adrenal; Adrenalectomy; Adrenocortical carcinoma; Adult; Anthracyclines; Asthenia; CT scan; Calretinin*; Cisplatin; Cyclophosphamide*; Dacarbazine; Doxorubicin; Endoscopy; Etoposide; Female; Flushing; Gallium scan; Genetics; Haematoxylin and eosin staining; Headache; Histopathology; Hypertension; Immunohistochemistry; January; KI-67*; Lynch Syndrome*; MRI; Mitotane; Oncology; PET scan; Pathology; Pembrolizumab*; Resection of tumour; SF-1*; Sandostatin*; Statins; Synaptophysin; Thorascopic surgery*; Ultrasound scan; Unique/unexpected symptoms or presentations of a disease; United States; Vimentin*; Vincristine*; White.
Figures
References
-
- Plager JE. Carcinoma of the adrenal cortex: clinical description, diagnosis, and treatment. International Advances in Surgical Oncology 1984. 329–353. - PubMed
-
- Challis BG, Kandasamy N, Powlson AS, Koulouri O, Annamalai AK, Happerfield L, Marker AJ, Arends MJ, Nik-Zainal S, Gurnell M. Familial adrenocortical carcinoma in association with Lynch syndrome. Journal of Clinical Endocrinology and Metabolism 2016. 2269–2272. (10.1210/jc.2016-1460) - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
