

The Partnership to Improve Diabetes Education Trial: a Cluster Randomized Trial Addressing Health Communication in Diabetes Care
- PMID: 31919724
- PMCID: PMC7174470
- DOI: 10.1007/s11606-019-05617-z
The Partnership to Improve Diabetes Education Trial: a Cluster Randomized Trial Addressing Health Communication in Diabetes Care
Abstract
Background: Effective type 2 diabetes care remains a challenge for patients including those receiving primary care in safety net settings.
Objective: The Partnership to Improve Diabetes Education (PRIDE) trial team and leaders from a regional department of health evaluated approaches to improve care for vulnerable patients.
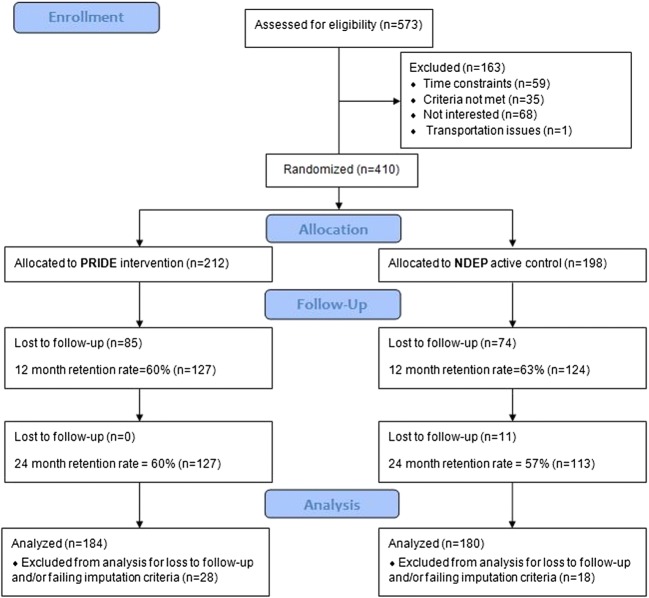
Design: Cluster randomized controlled trial.
Patients: Adults with uncontrolled type 2 diabetes seeking care across 10 unblinded, randomly assigned safety net clinics in Middle TN.
Interventions: A literacy-sensitive, provider-focused, health communication intervention (PRIDE; 5 clinics) vs. standard diabetes education (5 clinics).
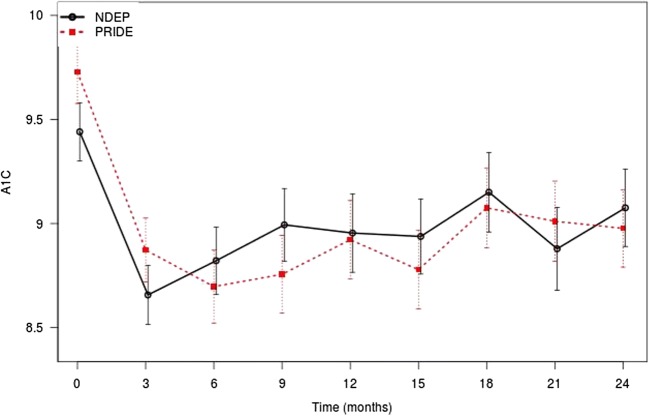
Main measures: Participant-level primary outcome was glycemic control [A1c] at 12 months. Secondary outcomes included select health behaviors and psychosocial aspects of care at 12 and 24 months. Adjusted mixed effects regression models were used to examine the comparative effectiveness of each approach to care.
Key results: Of 410 patients enrolled, 364 (89%) were included in analyses. Median age was 51 years; Black and Hispanic patients represented 18% and 25%; 96% were uninsured, and 82% had low annual income level (< $20,000); adequate health literacy was seen in 83%, but numeracy deficits were common. At 12 months, significant within-group treatment effects occurred from baseline for both PRIDE and control sites: adjusted A1c (- 0.76 [95% CI, - 1.08 to - 0.44]; P < .001 vs - 0.54 [95% CI, - 0.86 to - 0.21]; P = .001), odds of poor eating (0.53 [95% CI, 0.33-0.83]; P = .01 vs 0.42 [95% CI, 0.26-0.68]; P < .001), treatment satisfaction (3.93 [95% CI, 2.48-6.21]; P < .001 vs 3.04 [95% CI, 1.93-4.77]; P < .001), and self-efficacy (2.97 [95% CI, 1.89-4.67]; P < .001 vs 1.81 [95% CI, 1.1-2.84]; P = .01). No significant difference was observed between study arms in adjusted analyses.
Conclusions: Both interventions improved the participant's A1c and behavioral outcomes. PRIDE was not more effective than standard education. Further research may elucidate the added value of a focused health communication program in this setting.
Keywords: diabetes care; disparities; health communication; public health; vulnerable populations.
Conflict of interest statement
Dr. Rothman is a consultant for edLogics and Abbott, unrelated to the current project.
Figures
Comment in
-
Capsule Commentary on White et al., The Partnership to Improve Diabetes Education Trial: a Cluster Randomized Trial Addressing Health Communication in Diabetes Care.J Gen Intern Med. 2020 Apr;35(4):1357. doi: 10.1007/s11606-020-05662-z. J Gen Intern Med. 2020. PMID: 31965529 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention: National Diabetes Statistics Report. Atlanta (GA), Centers for Disease Control and Prevention, US Department of Health and Human Services, 2017, p. 20
-
- Ali MK, McKeever Bullard K, Imperatore G, Barker L, Gregg EW. Centers for Disease C, Prevention: Characteristics associated with poor glycemic control among adults with self-reported diagnosed diabetes--National Health and Nutrition Examination Survey, United States, 2007-2010. MMWR Suppl. 2012;61:32–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
