

Surgical Treatment of Chronic Rupture of the Quadriceps Using a Modified Pulvertaft Weave Technique
- PMID: 31921591
- PMCID: PMC6950773
- DOI: 10.1016/j.eats.2019.06.006
Surgical Treatment of Chronic Rupture of the Quadriceps Using a Modified Pulvertaft Weave Technique
Abstract
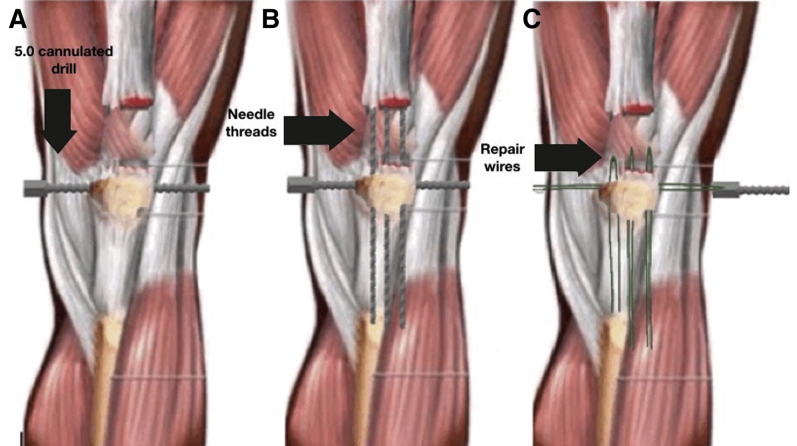
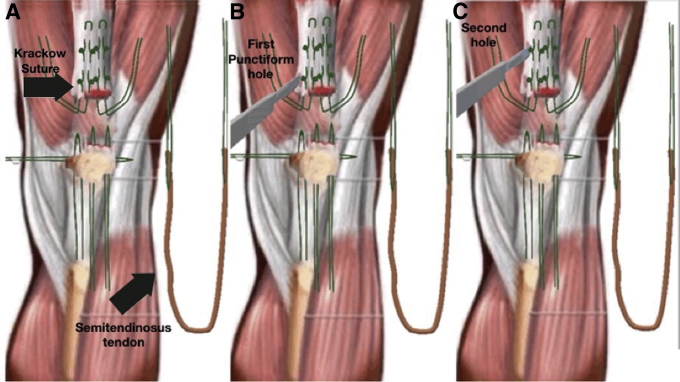
The extensor mechanism provides active knee joint extension and stability of the patellofemoral joint. Rupture of the quadriceps tendon, although uncommon, is therefore associated with impairment in knee joint stability and, thus, requires surgical repair. Although various techniques provide excellent clinical outcomes for acute rupture, treatment of chronic rupture remains clinically challenging. We describe our modified technique for quadriceps tendon repair using a semitendinosus tendon autograft, with suturing of the quadriceps tendon stump to the patella via transosseous sutures, wherein the use of allograft and anchors is avoided. Our modified Pulvertaft weave technique is simple and reproducible.
© 2019 by the Arthroscopy Association of North America. Published by Elsevier.
Figures




References
-
- Andrikoula S., Tokis A., Vasiliadis H.S., Georgoulis A. The extensor mechanism of the knee joint: An anatomical study. Knee Surg Sports Traumatol Arthrosc. 2006;14:214–220. - PubMed
-
- McGregory J.E. Disruption of the extensor mechanism of the knee. J Emerg Med. 2003;24:163–168. - PubMed
-
- Siwek C.W., Rao J.P. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63:932–937. - PubMed
LinkOut - more resources
Full Text Sources
