

Lymph Node Metastasis From Gastroesophageal Cancer Successfully Treated by Nivolumab: A Case Report of a Young Patient
- PMID: 31921639
- PMCID: PMC6927466
- DOI: 10.3389/fonc.2019.01375
Lymph Node Metastasis From Gastroesophageal Cancer Successfully Treated by Nivolumab: A Case Report of a Young Patient
Abstract
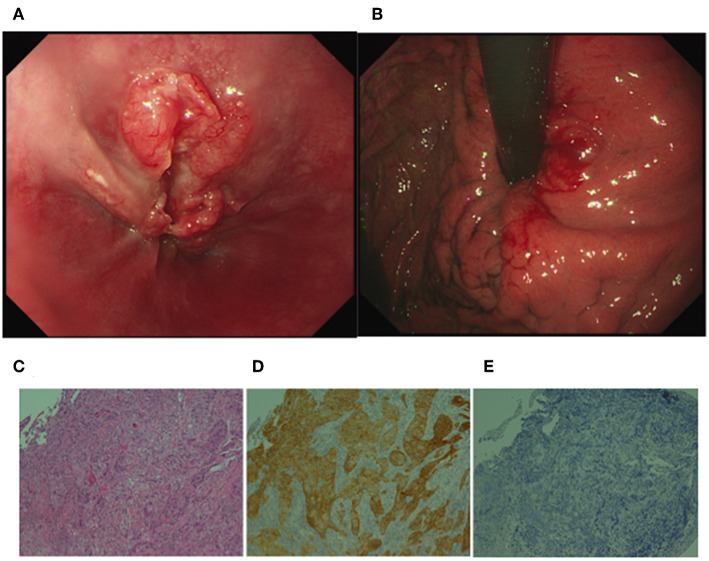
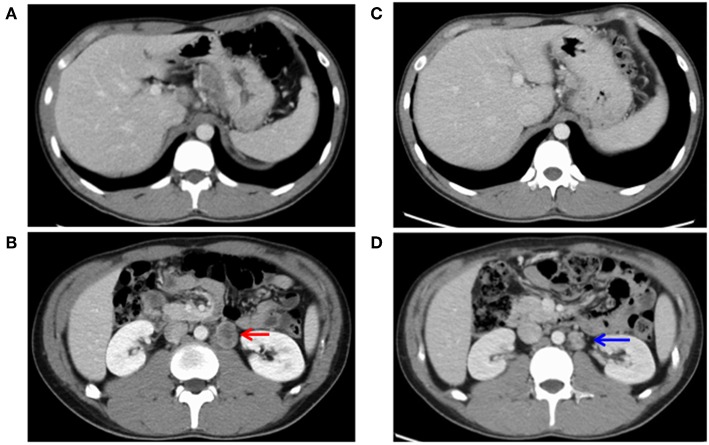
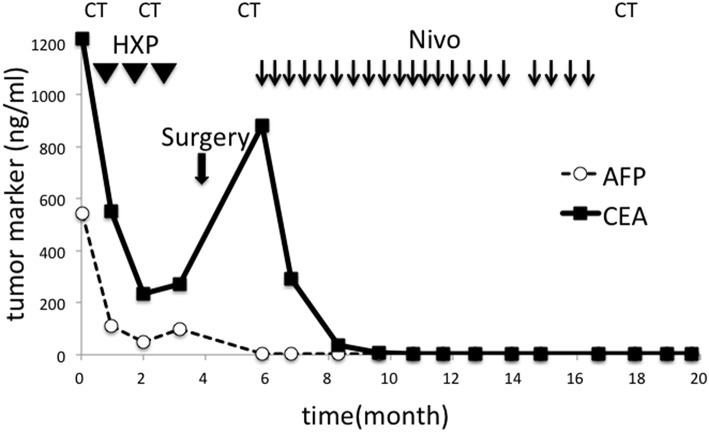
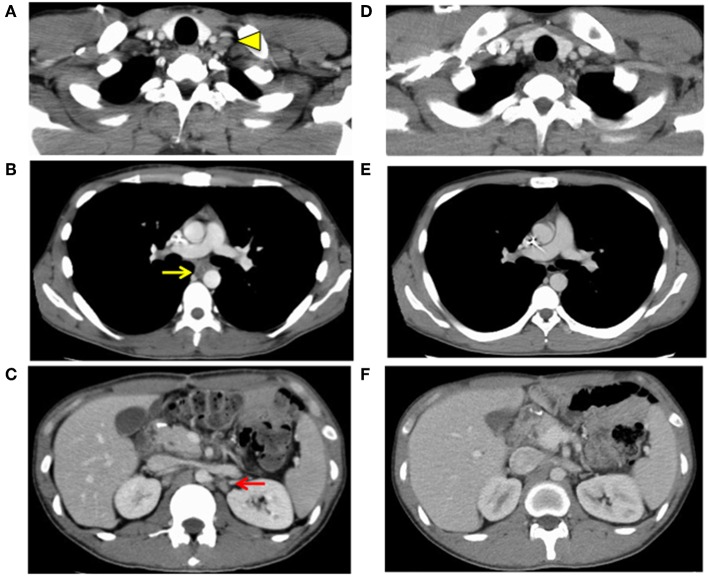
Background: Immuno-oncology is a novel target of cancer therapy. Nivolumab is a monoclonal anti-programed death-1 antibody recently used to treat patients with chemotherapy-resistant gastric and gastroesophageal cancer. Although the disease control rate is reported to be very high, few cases demonstrate a complete response. Case Presentation: A 25-year-old man diagnosed with gastroesophageal cancer was treated with chemotherapy followed by surgical resection. Pathological diagnosis was poorly differentiated adenocarcinoma with distant lymph node metastasis. Residual lymph node metastasis was treated with nivolumab monotherapy, resulting in complete disappearance. No recurrence has been observed for 2 years since discontinuation of nivolumab. This rare case was additionally subjected to pathological and genetic analysis, suggesting that a high tumor mutation burden (10.7 mutations/Mb) might be associated with sensitivity to nivolumab. Summary: We reported a case of advanced gastroesophageal junction cancer with distal lymph node metastasis that was successfully treated with chemotherapy, surgical resection, and nivolumab therapy. An aggressive search for biomarkers implying benefit effects of nivolumab should be performed.
Keywords: complete remission (CR); gastric cancer; immunotherapy; lymph node metastasis (LNM); tumor burden.
Copyright © 2019 Kashima, Tanabe, Tanino, Kobayashi, Murakami, Iwama, Sasaki, Kunogi, Takahashi, Ando, Ueno, Moriichi, Fukudo, Tasaki, Hosokawa, Mizukami, Fujiya and Okumura.
Figures
References
-
- Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. CONCORD Working Group. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. (2018) 391:1023–75. 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
-
- Kang YK, Boku N, Satoh T, Ryu MH, Chao Y, Kato K, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538–12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2017) 390:2461–71. 10.1016/S0140-6736(17)31827-5 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous