

Tracheomalacia and Tracheobronchomalacia in Pediatrics: An Overview of Evaluation, Medical Management, and Surgical Treatment
- PMID: 31921725
- PMCID: PMC6922019
- DOI: 10.3389/fped.2019.00512
Tracheomalacia and Tracheobronchomalacia in Pediatrics: An Overview of Evaluation, Medical Management, and Surgical Treatment
Abstract
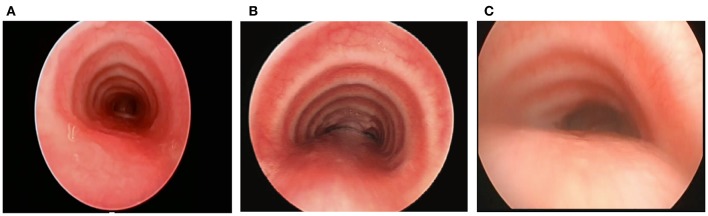
Tracheobronchomalacia (TBM) refers to airway collapse due to typically excessive posterior membrane intrusion and often associated with anterior cartilage compression. TBM occurs either in isolation or in association with other congenital or acquired conditions. Patients with TM typically present non-specific respiratory symptoms, ranging from noisy breathing with a typical barking cough to respiratory distress episodes to acute life-threatening events and recurrent and/or prolonged respiratory infections. There are no definitive standardized guidelines for the evaluation, diagnosis, and treatment of TBM; therefore, patients may be initially misdiagnosed and incorrectly treated. Although milder cases of TBM may become asymptomatic as the diameter of the airway enlarges with the child, in cases of severe TBM, more aggressive management is warranted. This article is an overview of the clinical presentation, evaluation, diagnosis, medical management, and surgical treatment options in pediatric tracheomalacia.
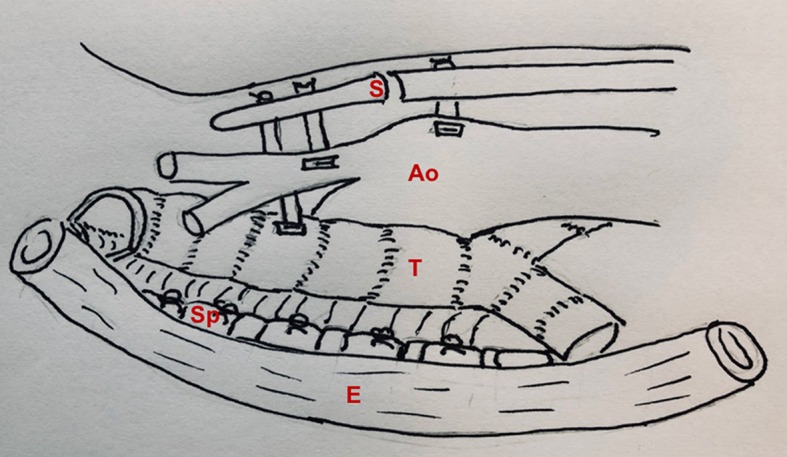
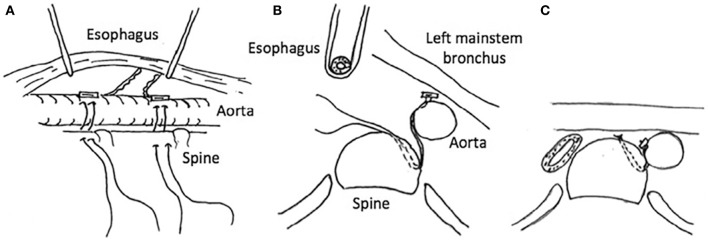
Keywords: aortopexy; tracheobronchomalacia; tracheobronchopexy; tracheomalacia; tracheopexy.
Copyright © 2019 Kamran and Jennings.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources