

A Combination Therapy for Kawasaki Disease with Severe Complications: a Case Report
- PMID: 31922014
- PMCID: PMC6944459
- DOI: 10.1515/med-2020-0002
A Combination Therapy for Kawasaki Disease with Severe Complications: a Case Report
Abstract
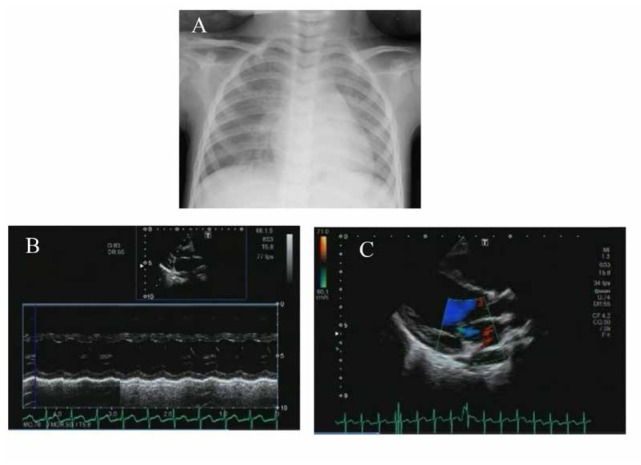
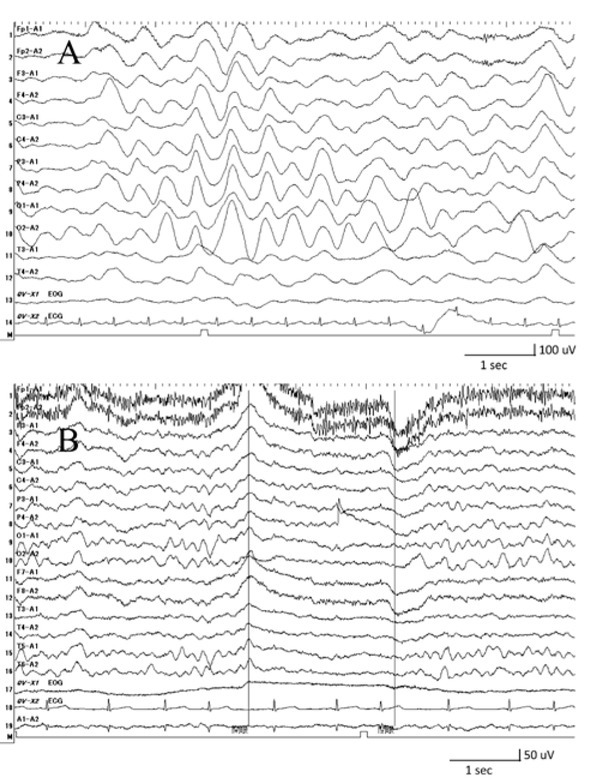
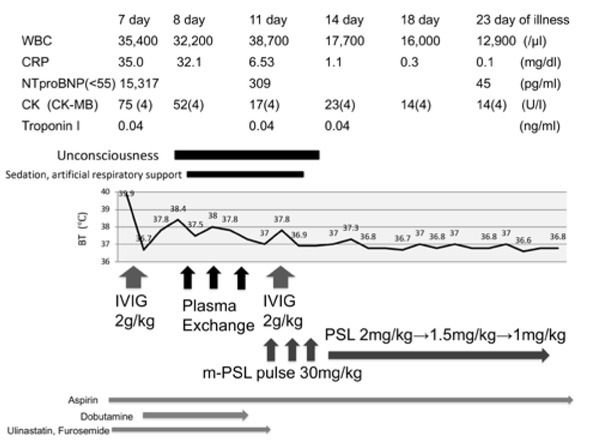
Kawasaki disease (KD) is a form of acute multisystem vasculitis that presents with various complications, including coronary artery aneurysm. Heart failure and brain damage are rare, but life-threatening complications are associated with KD. Here, we describe a 4-year-old girl who developed intravenous immunoglobulin-resistant KD with both left ventricular failure and acute encephalopathy. On day 8 of the illness, the low left ventricular ejection fraction, mitral regurgitation, and low blood pressure, which required continuous administration of dobutamine, were observed during the treatments for KD, including intravenous immunoglobulin. She also appeared unconscious, where the electroencephalogram showed slow waves of activity in all regions of the brain. The cardiac performance improved after she received plasma exchange for three days. However, her unconsciousness with slow waves of activity on electroencephalogram and fever continued after the plasma exchange. Therefore, she was treated with methylprednisolone pulse, followed by prednisolone, as well as intravenous immunoglobulin. Finally, she recovered without any cardiac or neurological sequelae not only at the time she was discharged, but also throughout the follow-up period. The combination therapy using plasma exchange and methylprednisolone pulse may be a treatment option for severe KD with left ventricular failure and acute encephalopathy complications.
Keywords: Combination therapy; Intravenous immunoglobulin-resistant Kawasaki disease; Methylprednisolone pulse; Plasma exchange.
© 2020 Yuriko Abe et al., published by De Gruyter.
Conflict of interest statement
Conflict of interest: Authors state no conflict of interest in this report.
Figures
Similar articles
-
[Effective therapy with infliximab for clinically mild encephalitis/encephalopathy with a reversible splenial lesion in an infant with Kawasaki disease].Nihon Rinsho Meneki Gakkai Kaishi. 2017;40(3):190-195. doi: 10.2177/jsci.40.190. Nihon Rinsho Meneki Gakkai Kaishi. 2017. PMID: 28747606 Japanese.
-
Kawasaki disease involving both the nervous system and cardiovascular system: a case report and literature review.Front Pediatr. 2024 Dec 2;12:1459143. doi: 10.3389/fped.2024.1459143. eCollection 2024. Front Pediatr. 2024. PMID: 39687711 Free PMC article.
-
A case of incomplete Kawasaki disease - A 2-month-old infant with 1 day of fever who developed multiple arterial aneurysms.Ann Pediatr Cardiol. 2022 Sep-Dec;15(5-6):536-538. doi: 10.4103/apc.apc_39_22. Epub 2023 Mar 1. Ann Pediatr Cardiol. 2022. PMID: 37152506 Free PMC article.
-
[Kawasaki disease: what you need to know].Arch Pediatr. 2012 Nov;19(11):1264-8. doi: 10.1016/j.arcped.2012.07.005. Epub 2012 Aug 24. Arch Pediatr. 2012. PMID: 22921712 Review. French.
-
History and Future of Treatment for Acute Stage Kawasaki Disease.Korean Circ J. 2020 Feb;50(2):112-119. doi: 10.4070/kcj.2019.0290. Epub 2019 Dec 3. Korean Circ J. 2020. PMID: 31845551 Free PMC article. Review.
References
-
- Lue H.C., Chen L.R., Lin M.T., Chang L.Y., Wang J.K., Lee C.Y.. Estimation of the incidence of Kawasaki disease in Taiwan. A comparison of two data sources: nationwide hospital survey and national health insurance claims. Pediatr Neonatol. 2014;55:97–100. doi: 10.1016/j.pedneo.2013.05.011. et al. - DOI - PubMed
LinkOut - more resources
Full Text Sources