

Predicting and Defining Steroid Resistance in Pediatric Nephrotic Syndrome Using Plasma Proteomics
- PMID: 31922062
- PMCID: PMC6943770
- DOI: 10.1016/j.ekir.2019.09.009
Predicting and Defining Steroid Resistance in Pediatric Nephrotic Syndrome Using Plasma Proteomics
Abstract
Introduction: Nephrotic syndrome (NS) is a characterized by massive proteinuria, edema, hypoalbuminemia, and dyslipidemia. Glucocorticoids (GCs), the primary therapy for >60 years, are ineffective in approximately 50% of adults and approximately 20% of children. Unfortunately, there are no validated biomarkers able to predict steroid-resistant NS (SRNS) or to define the pathways regulating SRNS.
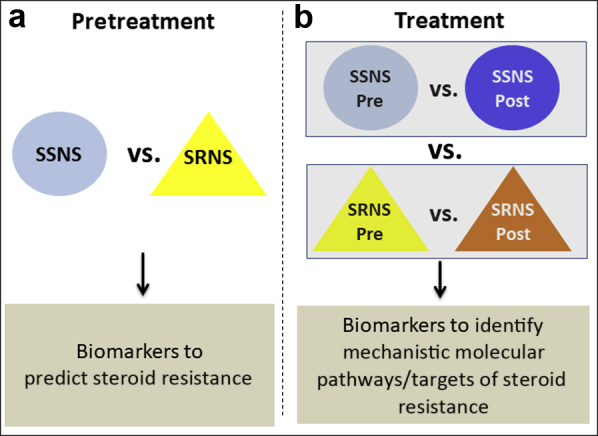
Methods: We performed proteomic analyses on paired pediatric NS patient plasma samples obtained both at disease presentation before glucocorticoid initiation and after approximately 7 weeks of GC therapy to identify candidate biomarkers able to either predict steroid resistance before treatment or define critical molecular pathways/targets regulating steroid resistance.
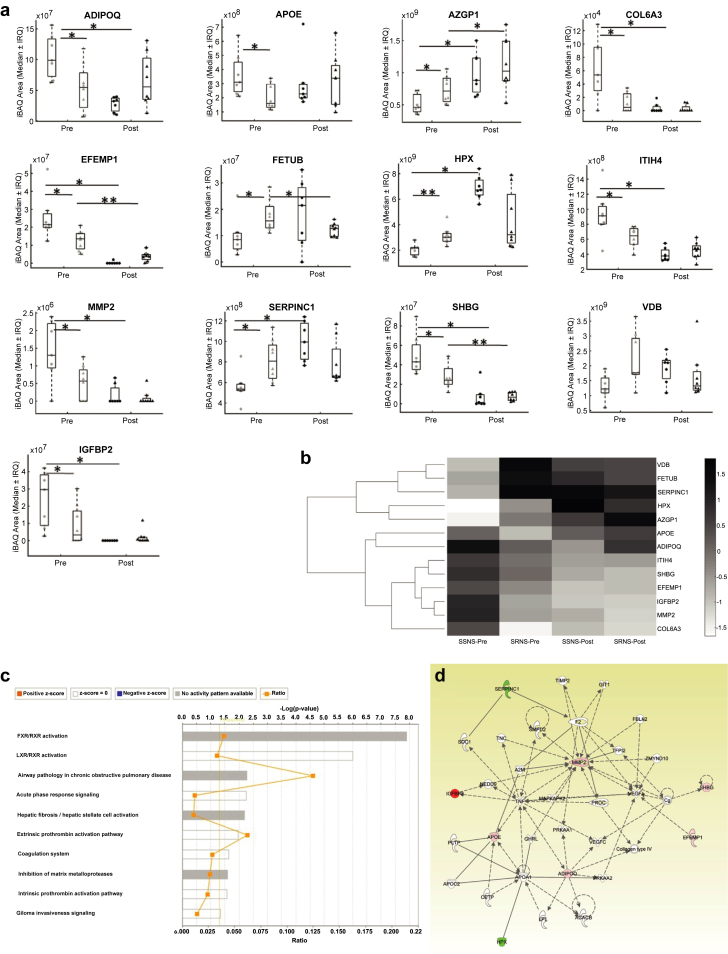
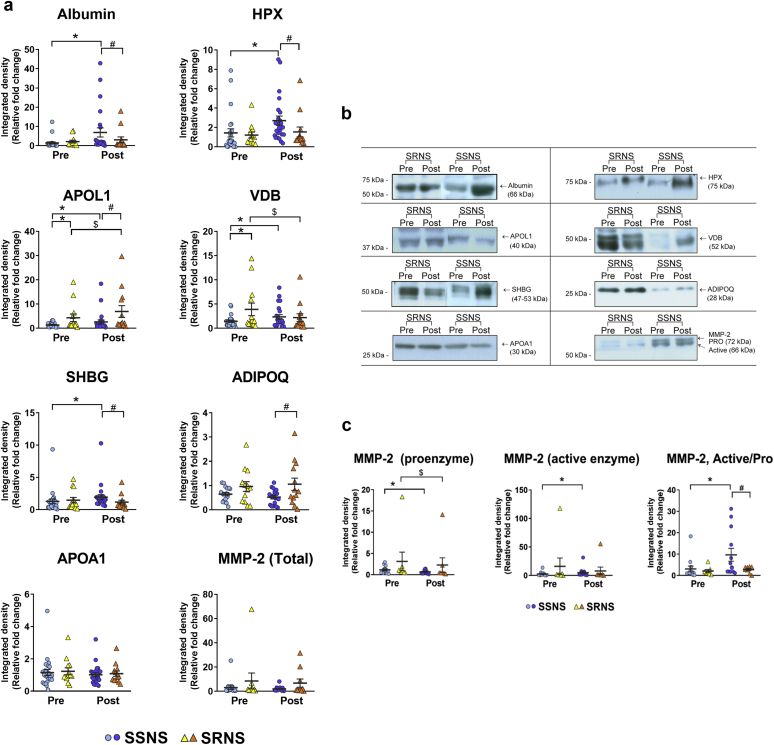
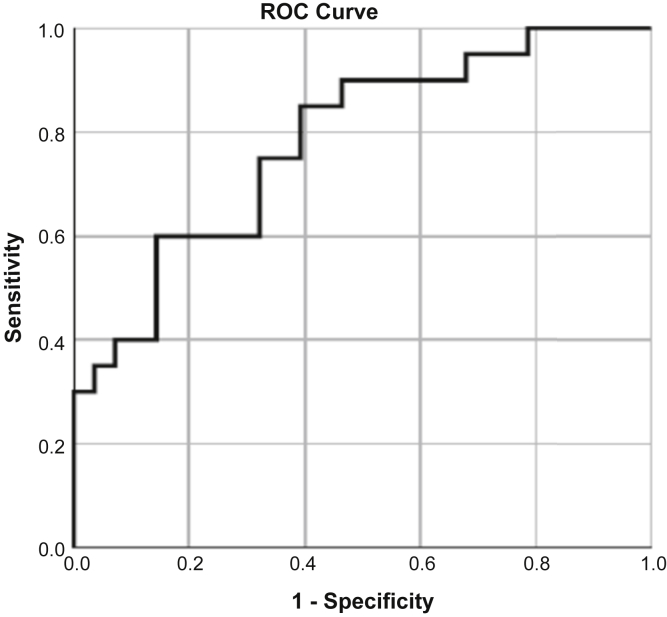
Results: Proteomic analyses of 15 paired NS patient samples identified 215 prevalent proteins, including 13 candidate biomarkers that predicted SRNS before GC treatment, and 66 candidate biomarkers that mechanistically differentiated steroid-sensitive NS (SSNS) from SRNS. Ingenuity Pathway Analyses and protein networking pathways approaches further identified proteins and pathways associated with SRNS. Validation using 37 NS patient samples (24 SSNS/13 SRNS) confirmed vitamin D binding protein (VDB) and APOL1 as strong predictive candidate biomarkers for SRNS, and VDB, hemopexin (HPX), adiponectin (ADIPOQ), sex hormone-binding globulin (SHBG), and APOL1 as strong candidate biomarkers to mechanistically distinguish SRNS from SSNS. Logistic regression analysis identified a candidate biomarker panel (VDB, ADIPOQ, and matrix metalloproteinase 2 [MMP-2]) with significant ability to predict SRNS at disease presentation (P = 0.003; area under the receiver operating characteristic curve = 0.78).
Conclusion: Plasma proteomic analyses and immunoblotting of serial samples in childhood NS identified a candidate biomarker panel able to predict SRNS at disease presentation, as well as candidate molecular targets/pathways associated with clinical steroid resistance.
Keywords: biomarkers; nephrotic syndrome; proteomics; steroid resistance.
© 2019 International Society of Nephrology. Published by Elsevier Inc.
Figures
Comment in
-
Predictive Biomarkers in Nephrology Around the Corner.Kidney Int Rep. 2019 Nov 2;5(1):1-3. doi: 10.1016/j.ekir.2019.10.009. eCollection 2020 Jan. Kidney Int Rep. 2019. PMID: 31930209 Free PMC article. No abstract available.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
