

The Molecular Analysis for Therapy Choice (NCI-MATCH) Trial: Lessons for Genomic Trial Design
- PMID: 31922567
- PMCID: PMC7566320
- DOI: 10.1093/jnci/djz245
The Molecular Analysis for Therapy Choice (NCI-MATCH) Trial: Lessons for Genomic Trial Design
Erratum in
-
Corrigendum to: The Molecular Analysis for Therapy Choice (NCI-MATCH) Trial: Lessons for Genomic Trial Design.J Natl Cancer Inst. 2022 Feb 7;114(2):325. doi: 10.1093/jnci/djab115. J Natl Cancer Inst. 2022. PMID: 34418051 Free PMC article. No abstract available.
Abstract
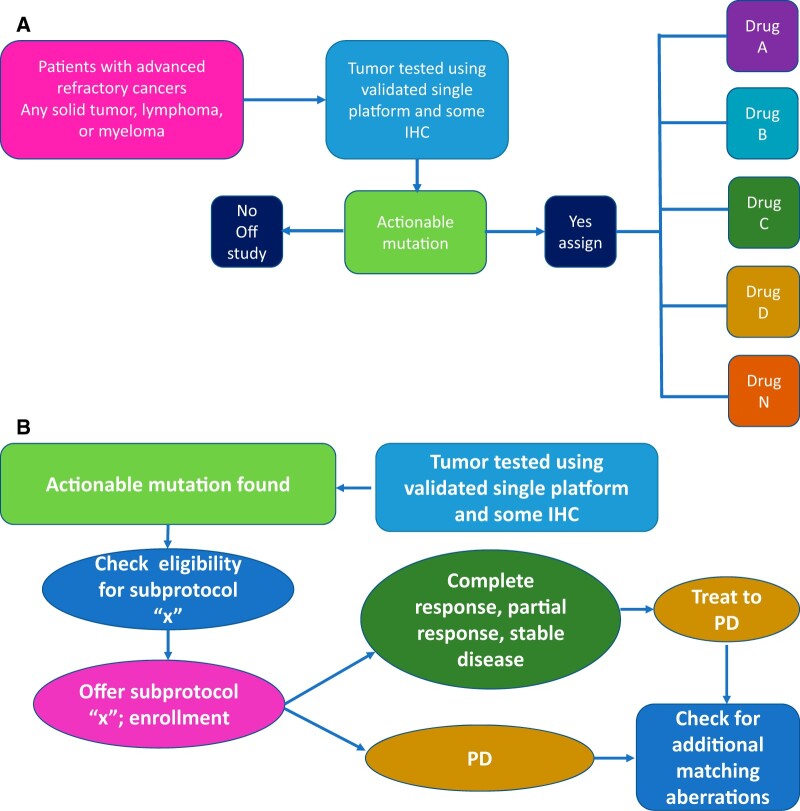
Background: The proportion of tumors of various histologies that may respond to drugs targeted to molecular alterations is unknown. NCI-MATCH, a collaboration between ECOG-ACRIN Cancer Research Group and the National Cancer Institute, was initiated to find efficacy signals by matching patients with refractory malignancies to treatment targeted to potential tumor molecular drivers regardless of cancer histology.
Methods: Trial development required assumptions about molecular target prevalence, accrual rates, treatment eligibility, and enrollment rates as well as consideration of logistical requirements. Central tumor profiling was performed with an investigational next-generation DNA-targeted sequencing assay of alterations in 143 genes, and protein expression of protein expression of phosphatase and tensin homolog, mutL homolog 1, mutS homolog 2, and RB transcriptional corepressor 1. Treatments were allocated with a validated computational platform (MATCHBOX). A preplanned interim analysis evaluated assumptions and feasibility in this novel trial.
Results: At interim analysis, accrual was robust, tumor biopsies were safe (<1% severe events), and profiling success was 87.3%. Actionable molecular alteration frequency met expectations, but assignment and enrollment lagged due to histology exclusions and mismatch of resources to demand. To address this lag, we revised estimates of mutation frequencies, increased screening sample size, added treatments, and improved assay throughput and efficiency (93.9% completion and 14-day turnaround).
Conclusions: The experiences in the design and implementation of the NCI-MATCH trial suggest that profiling from fresh tumor biopsies and assigning treatment can be performed efficiently in a large national network trial. The success of such trials necessitates a broad screening approach and many treatment options easily accessible to patients.
© The Author(s) 2019. Published by Oxford University Press.
Figures

References
-
- Cortesi L, De Matteis E, Cirilli C, Marcheselli L, Proietto M, Federico M.. Outcome evaluation in pre-trastuzumab era between different breast cancer phenotypes: a population-based study on Italian women. Tumori. 2012;98(6):743–750. - PubMed
-
- Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. - PubMed
-
- Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–1500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
